
Behavior Therapy & CBT
Comprehensive Nursing Notes on Behavioral & Cognitive Approaches
Introduction to Behavioral Approaches
Behavioral and cognitive-behavioral therapies are evidence-based approaches used to treat a variety of mental health conditions. These therapeutic modalities focus on identifying and modifying maladaptive thoughts and behaviors to improve psychological well-being.
Behavioral Therapy
Focused on the principles that behaviors are learned and can be modified without necessarily addressing underlying thoughts. Rooted in classical and operant conditioning.
Cognitive Behavioral Therapy
Integrates behavioral principles with cognitive psychology to address both thoughts and behaviors. Focuses on the relationship between thoughts, feelings, and behaviors.
Clinical Pearl
Both approaches are action-oriented and goal-focused, making them well-suited for the nursing process with their emphasis on measurable outcomes and evidence-based interventions.
Behavioral Therapy: Principles & Foundation
Historical Context
Behavioral therapy emerged in the early 20th century, pioneered by figures like John B. Watson and B.F. Skinner. It represented a departure from psychoanalytic approaches by focusing on observable behaviors rather than unconscious processes.
Core Assumption of Behavioral Therapy
Maladaptive behaviors are learned responses to environmental stimuli and can be unlearned or replaced through the application of learning principles.
Classical Conditioning

Involves forming associations between stimuli. A previously neutral stimulus is paired with a stimulus that naturally evokes a response. After repeated pairings, the neutral stimulus alone can trigger the response.
- Unconditioned Stimulus (UCS): Naturally triggers a response
- Unconditioned Response (UCR): Natural response to UCS
- Conditioned Stimulus (CS): Initially neutral stimulus
- Conditioned Response (CR): Learned response to CS
Operant Conditioning

Focuses on how consequences influence behaviors. Behaviors followed by desirable consequences are more likely to be repeated, while those followed by negative consequences are less likely to recur.
- Reinforcement: Increases behavior frequency
- Punishment: Decreases behavior frequency
- Extinction: Removal of reinforcement to eliminate behavior
- Shaping: Reinforcing successive approximations toward desired behavior
Key Principles of Behavioral Therapy
Focus on Present
Addresses current problems rather than exploring past experiences
Observable Behaviors
Targets behaviors that can be clearly defined and measured
Learning Principles
Applies theories of how behaviors are acquired and maintained
Specific Goals
Sets clear, measurable objectives for behavior change
Environmental Focus
Considers how environment shapes and maintains behaviors
Empirical Approach
Emphasizes evidence-based practices and measurable outcomes
Mnemonic: “SAMPLE” for Behavioral Therapy Principles
- Specific behavior focus
- Action-oriented approach
- Measurable outcomes
- Present-centered (not past-focused)
- Learning principles application
- Environmental modifications
Behavioral Therapy Techniques
Classical Conditioning Techniques
Systematic Desensitization
Gradually exposing clients to anxiety-provoking stimuli while teaching relaxation techniques. Particularly effective for phobias and anxiety disorders.
- Create anxiety hierarchy (least to most anxiety-provoking)
- Teach relaxation techniques
- Gradually expose to items on hierarchy while relaxed
- Progress when comfort is established at each level
Flooding
Intense exposure to fear-inducing stimuli with prevention of avoidance, leading to extinction of fear response. More rapid than systematic desensitization but potentially more distressing.
Aversion Therapy
Pairing an undesirable behavior with an aversive stimulus to reduce the behavior’s frequency.
Operant Conditioning Techniques
Positive Reinforcement
Providing rewards or pleasant outcomes after desired behaviors to increase their frequency.
Token Economy
A system where clients earn tokens for positive behaviors, which can later be exchanged for privileges or rewards.
- Define target behaviors clearly
- Establish token values for each behavior
- Create a “menu” of rewards with costs
- Consistently implement token distribution
- Regularly review and adjust as needed
Extinction & Time-Out
Extinction involves withholding reinforcement to reduce unwanted behaviors. Time-out removes the person from reinforcing environments.
- Extinction burst: Behavior often increases before decreasing
- Consistency is essential for effectiveness
- Time-out should be brief and age-appropriate
- Follow-up with teaching alternative behaviors
Additional Behavioral Techniques
Behavioral Contracting
Formal written agreement between client and clinician outlining behavior goals, reinforcements, and consequences.
Modeling
Learning through observation and imitation of others demonstrating desired behaviors.
Behavior Shaping
Reinforcing successive approximations of desired behavior until the target behavior is achieved.
Behavior Chaining
Breaking complex behaviors into smaller steps and teaching each step sequentially.
Self-Monitoring
Teaching clients to observe and record their own behaviors to increase awareness.
Social Skills Training
Structured practice of interpersonal behaviors through role-play and feedback.
Mnemonic: “PRIME” for Behavioral Techniques
- Positive reinforcement & Punishment procedures
- Relaxation training (in systematic desensitization)
- Imitation through modeling
- Monitoring behavior (self-monitoring)
- Exposure techniques (systematic desensitization, flooding)
Cognitive Behavioral Therapy (CBT)
Development & Foundation
Cognitive Behavioral Therapy (CBT) was developed in the 1960s by Aaron Beck, who recognized that depression involved distorted thinking patterns. CBT integrates behavioral principles with an emphasis on how cognitions (thoughts) influence emotions and behaviors.

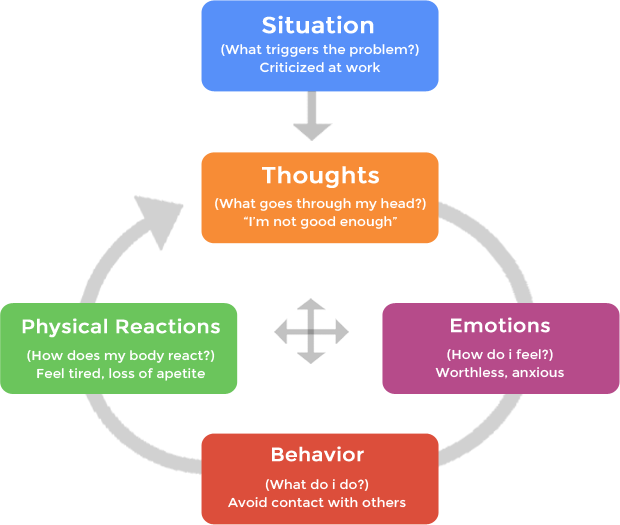
The CBT Triangle: Thoughts, Feelings, and Behaviors are interconnected
Core Assumption of CBT
Psychological distress is maintained by cognitive factors, and individuals can learn to identify, evaluate, and modify these thoughts and the associated behaviors.
CBT Model & Key Components
Automatic Thoughts
Immediate, unpremeditated interpretations of events that shape emotional and behavioral responses.
If a friend passes you without saying hello:
- Negative automatic thought: “They’re ignoring me; they must be angry with me.”
- Alternative thought: “They might be preoccupied or didn’t see me.”
Cognitive Distortions
Errors in thinking that reinforce negative thought patterns and lead to psychological distress.
- All-or-nothing thinking
- Overgeneralization
- Mental filtering
- Catastrophizing
- Emotional reasoning
- Should statements
Core Beliefs
Fundamental, deeply held beliefs about oneself, others, and the world that influence automatic thoughts and behaviors.
- Core beliefs: “I am unlovable” or “The world is dangerous”
- Intermediate beliefs: Rules, attitudes, and assumptions like “I must always please others to be accepted”
The CBT Process Model

Components and process of Cognitive Behavioral Therapy
Mnemonic: “ABCDE” for the CBT Process
- Activating event (situation or trigger)
- Beliefs and thoughts about the event
- Consequences (emotional and behavioral)
- Disputing irrational beliefs
- Effective new philosophy or approach
CBT Techniques & Strategies
Cognitive Techniques
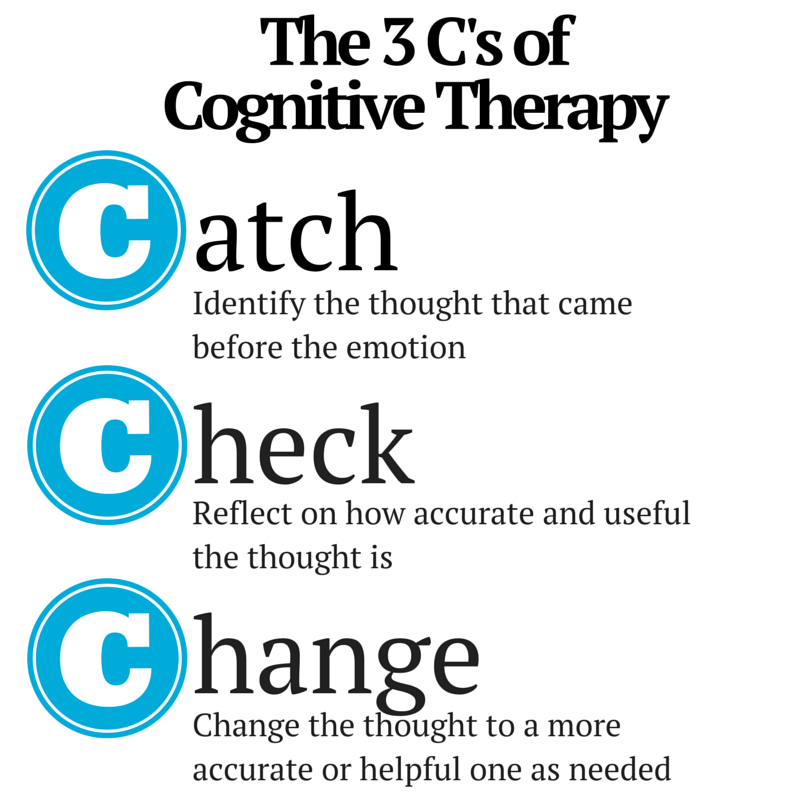
Cognitive Restructuring
Identifying, challenging, and modifying negative or distorted thoughts with more balanced, realistic alternatives.
- Catch the negative thought
- Check the evidence for and against it
- Change to a more balanced perspective
Thought Records
Structured worksheets where clients document situations, automatic thoughts, emotions, and alternative perspectives.
| Situation | Automatic Thought | Emotion & Intensity | Alternative Thought |
|---|---|---|---|
| Failed exam | “I’m stupid” | Sadness (8/10) | “One exam doesn’t define my intelligence” |
Socratic Questioning
Using guided questions to help clients examine the evidence, assumptions, and consequences of their thoughts.
- “What evidence supports this thought?”
- “What would you tell a friend in this situation?”
- “Are you looking at the whole picture?”
- “How else could you interpret this situation?”
- “What are the costs and benefits of thinking this way?”
Behavioral Techniques in CBT
Behavioral Experiments
Structured activities designed to test the validity of beliefs or fears and gather new evidence.
Activity Scheduling
Planning and engaging in pleasurable and mastery activities, especially helpful for depression.
- Gentleness with self
- Relaxation
- Accomplishment
- Pleasure
- Exercise
- Socializing
Exposure Techniques
Gradual, controlled exposure to feared situations or stimuli, combined with cognitive techniques.
- In vivo exposure: Real-life encounters with feared situations
- Imaginal exposure: Visualizing feared scenarios
- Interoceptive exposure: Deliberately inducing physical sensations associated with anxiety
CBT Session Structure & Process
Assessment & Conceptualization
Gather information about presenting problems, history, and develop a cognitive-behavioral case formulation.
Goal Setting
Collaboratively establish specific, measurable, achievable, relevant, and time-bound (SMART) goals.
Psychoeducation
Teach clients about the CBT model and how thoughts influence emotions and behaviors.
Skill Building
Teach cognitive and behavioral techniques tailored to the client’s specific needs.
Homework Assignments
Assign between-session practice of skills to reinforce learning and facilitate change.
Progress Monitoring
Regularly assess progress toward goals and adjust treatment as needed.
Relapse Prevention
Prepare for potential setbacks and develop strategies to maintain gains after treatment ends.
Clinical Pearl: Typical CBT Session Structure
- Brief mood check and update
- Bridge from previous session
- Homework review
- Collaborative agenda setting
- Discussion of agenda items using CBT techniques
- Homework assignment
- Session summary and feedback
Applications in Nursing Practice
Clinical Applications
Mental Health Conditions
Evidence-based applications of behavioral and cognitive therapies:
| Condition | Effective Approach |
|---|---|
| Depression | CBT with focus on negative thoughts, behavioral activation |
| Anxiety Disorders | CBT with exposure, cognitive restructuring |
| PTSD | Trauma-focused CBT, exposure therapy |
| OCD | Exposure and response prevention (ERP) |
| Substance Use | Behavioral therapy, coping skills training |
| Eating Disorders | CBT with focus on body image and eating behaviors |
Medical Conditions
Behavioral and cognitive approaches can help patients manage chronic conditions:
- Chronic pain management
- Medication adherence
- Stress reduction
- Sleep hygiene for insomnia
- Lifestyle modifications for diabetes, hypertension
- Coping with illness-related anxiety and depression
Nursing Implementation
Adapting Techniques for Nursing Settings
Nurses can incorporate elements of behavioral and cognitive approaches:
- Brief cognitive interventions during routine care
- Teaching relaxation techniques for anxiety or pain
- Using behavioral principles to encourage treatment adherence
- Implementing token economies in psychiatric settings
- Helping patients identify and challenge unhelpful thoughts
- Providing psychoeducation about the mind-body connection
Integration with Nursing Process
| Nursing Process Step | Behavioral/Cognitive Integration |
|---|---|
| Assessment | Evaluate thoughts, behaviors, and their relationship to symptoms |
| Diagnosis | Identify nursing diagnoses related to cognitive and behavioral patterns |
| Planning | Set measurable behavioral goals collaboratively with patient |
| Implementation | Apply appropriate cognitive and behavioral techniques |
| Evaluation | Monitor progress with objective behavioral measures |
Scope of Practice Consideration
While nurses can incorporate elements of these approaches, formal CBT typically requires specialized training. Always work within your scope of practice and refer to mental health specialists when appropriate.
Case Examples for Nursing Practice
Case 1: Anxiety in Medical Setting
Patient experiencing anticipatory anxiety before procedures.
- Teach diaphragmatic breathing for relaxation
- Help identify and challenge catastrophic thoughts
- Use systematic desensitization approach
- Provide accurate information to counter misconceptions
- Reinforce coping behaviors
Case 2: Medication Adherence
Patient struggling with consistent medication taking.
- Identify barriers and beliefs about medications
- Establish a behavioral contract
- Use reinforcement strategies
- Implement reminder systems and environmental cues
- Regular follow-up and positive reinforcement
Comparison of Approaches
Behavioral Therapy vs. Cognitive Behavioral Therapy
| Feature | Behavioral Therapy | Cognitive Behavioral Therapy |
|---|---|---|
| Focus | Observable behaviors | Thoughts, behaviors, and their interaction |
| Theoretical Foundation | Classical and operant conditioning | Learning theories plus cognitive model |
| Primary Mechanism of Change | Changing behavior directly through learning principles | Modifying thoughts to change emotions and behaviors |
| Assessment Focus | Behavioral analysis, antecedents, consequences | Thoughts, beliefs, behaviors, and their relationships |
| Core Techniques | Reinforcement, extinction, exposure, modeling | Cognitive restructuring, behavioral experiments, exposure |
| Approach to Inner Experience | Less emphasis on internal mental states | Directly addresses thoughts, beliefs, and interpretations |
| Most Effective For | Specific behavioral problems, phobias, habit disorders | Depression, anxiety, conditions with cognitive components |
| Client Role | Active participant in behavior change | Active collaborator in identifying and changing thoughts and behaviors |
| Timeline | Typically shorter term | Structured, time-limited (8-20 sessions typical) |
Specialized Variants of CBT
Dialectical Behavior Therapy (DBT)
Combines CBT with mindfulness and acceptance strategies. Particularly effective for emotional regulation and borderline personality disorder.
Acceptance and Commitment Therapy (ACT)
Emphasizes acceptance of thoughts and feelings while committing to behavior change aligned with values.
Trauma-Focused CBT
Adapted for addressing trauma-related symptoms, particularly in children and adolescents who have experienced trauma.
Clinical Pearl: Selecting the Right Approach
Consider using more purely behavioral approaches when:
- Working with young children or individuals with cognitive limitations
- Targeting specific, well-defined behaviors
- Immediate behavior management is needed
Consider CBT when:
- Negative thought patterns contribute significantly to the problem
- The client has sufficient cognitive abilities to identify and work with thoughts
- Long-term change and relapse prevention are priorities
Mnemonics & Memory Aids
Behavioral Therapy Memory Aids
“SAMPLE” – Principles of Behavioral Therapy
- Specific behavior focus
- Action-oriented approach
- Measurable outcomes
- Present-centered (not past-focused)
- Learning principles application
- Environmental modifications
“PRIME” – Behavioral Techniques
- Positive reinforcement & Punishment procedures
- Relaxation training (in systematic desensitization)
- Imitation through modeling
- Monitoring behavior (self-monitoring)
- Exposure techniques (systematic desensitization, flooding)
“FEAR” – Steps in Systematic Desensitization
- Fear hierarchy development
- Equip with relaxation techniques
- Alternating relaxation with exposure
- Repeat until desensitized
CBT Memory Aids
“ABCDE” – CBT Framework
- Activating event (situation)
- Beliefs about the event
- Consequences (emotional & behavioral)
- Disputing irrational beliefs
- Effective new philosophy
“3 C’s” – Cognitive Restructuring Process
- Catch the negative thought
- Check the evidence
- Change to a more balanced perspective
“GRAPES” – Activity Scheduling Categories
- Gentleness with self
- Relaxation
- Accomplishment
- Pleasure
- Exercise
- Socializing
Flowcharts & Visual Aids
CBT Conceptualization Flowchart
Common Cognitive Distortions
- All-or-Nothing Thinking: Seeing things in black-and-white categories
- Overgeneralization: Viewing a single negative event as a never-ending pattern
- Mental Filter: Focusing exclusively on negatives while filtering out positives
- Disqualifying the Positive: Rejecting positive experiences as “not counting”
- Jumping to Conclusions: Making negative interpretations without definite facts
- Catastrophizing: Expecting disaster; magnifying problems
- Emotional Reasoning: Believing something must be true because it “feels” true
- Should Statements: Using rigid rules about how people “should” behave
- Labeling: Attaching a negative label to yourself or others
- Personalization: Seeing yourself as the cause of external events
Summary & Key Takeaways
Behavioral Therapy
- Focuses on observable behaviors rather than internal mental processes
- Based on classical and operant conditioning principles
- Techniques include systematic desensitization, exposure, reinforcement strategies
- Particularly effective for specific behavioral issues and phobias
- Action-oriented and emphasizes measurable outcomes
- Can be implemented without addressing cognitive processes
Cognitive Behavioral Therapy
- Integrates behavioral and cognitive approaches
- Focuses on how thoughts influence emotions and behaviors
- Addresses automatic thoughts, cognitive distortions, and core beliefs
- Techniques include cognitive restructuring and behavioral experiments
- Effective for depression, anxiety, and various psychological disorders
- Structured, goal-oriented, and typically time-limited
Nursing Applications
- Elements of both approaches can be integrated into nursing care
- Useful for managing psychological aspects of medical conditions
- Can enhance medication adherence and lifestyle changes
- Structured approach aligns well with nursing process
- Can be incorporated into brief interventions during routine care
- Important to work within scope of practice and refer when appropriate
Final Clinical Pearl
While behavioral and cognitive approaches have distinct theoretical foundations, they complement each other in practice. The integration of both approaches provides a powerful framework for addressing a wide range of psychological and behavioral challenges encountered in nursing practice. Remember that these interventions are skills-based and require practice for both the nurse and the patient.