
Anesthesia in Nursing
Comprehensive Study Notes for Nursing Students
Types, Methods, Effects, Stages, Equipment & Drugs
Anesthesia Overview: Stages and Equipment
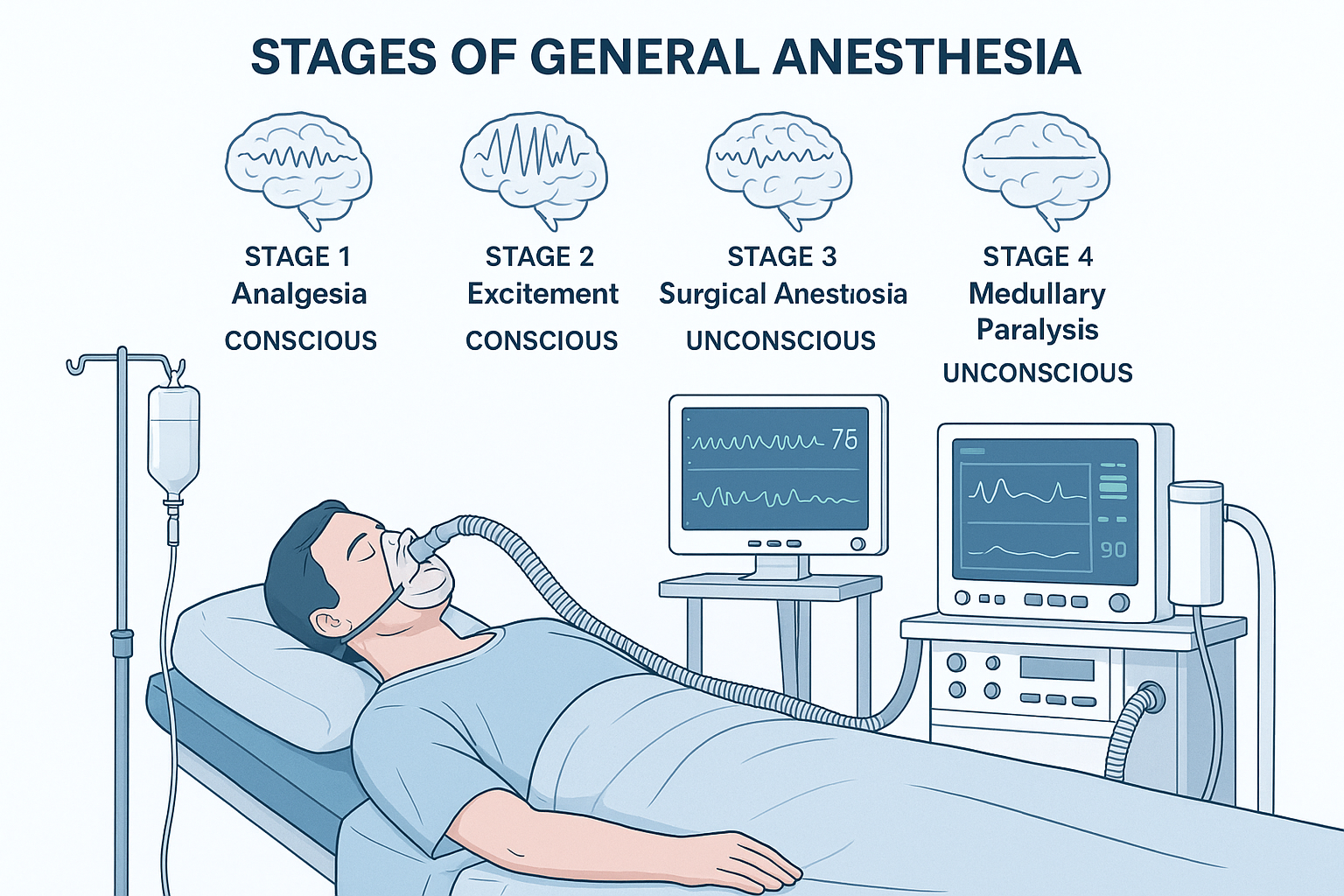
This illustration demonstrates the comprehensive anesthesia setup including monitoring equipment, ventilation systems, and the progression through anesthetic stages.
Table of Contents
Introduction to Anesthesia
Anesthesia is a medical intervention that temporarily eliminates or reduces sensation, particularly pain, to enable surgical procedures and other medical interventions. As a nursing professional, understanding anesthesia is crucial for providing comprehensive perioperative care and ensuring patient safety throughout the surgical experience.
Definition and Core Principles
Anesthesia derives from the Greek words “an” (without) and “aisthesis” (sensation). It encompasses three fundamental components:
- Analgesia: Absence of pain perception
- Amnesia: Loss of memory formation during the procedure
- Akinesia: Absence of movement and muscle relaxation
Memory Aid: The 3 A’s of Anesthesia
AAA – Remember the three core goals:
Analgesia
No Pain
Amnesia
No Memory
Akinesia
No Movement
Historical Context and Modern Practice
The evolution of anesthesia has revolutionized surgical practice since the first successful demonstration of ether anesthesia by William Morton in 1846. Today’s anesthetic practice integrates advanced pharmacology, sophisticated monitoring technology, and evidence-based protocols to ensure optimal patient outcomes while minimizing risks.
Modern anesthesia practice encompasses not only the intraoperative period but extends to preoperative optimization and postoperative recovery management. This comprehensive approach requires nurses to understand the entire perioperative continuum and their role in each phase.
Types of Anesthesia
General Anesthesia
Complete unconsciousness with muscle relaxation
Regional Anesthesia
Blocks sensation in specific body regions
Local Anesthesia
Numbs specific surgical site area
Sedation
Reduced consciousness with maintained reflexes
General Anesthesia
General anesthesia produces a controlled, reversible state of unconsciousness characterized by loss of sensation, awareness, and memory. It involves depression of the central nervous system to a degree that allows surgical procedures to be performed without patient discomfort or awareness.
Characteristics:
- Complete loss of consciousness
- Loss of protective reflexes
- Amnesia for the surgical period
- Muscle relaxation
- Requires airway management
- Hemodynamic stability maintenance
Indications:
- Major surgical procedures
- Operations requiring muscle relaxation
- Procedures in body cavities
- Patient positioning requirements
- Patient preference or anxiety
- Contraindications to regional techniques
Regional Anesthesia
Regional anesthesia involves blocking nerve conduction in a specific region of the body while maintaining consciousness. This technique provides excellent analgesia for procedures in the blocked region while preserving patient awareness and protective reflexes.
Spinal Anesthesia
- Local anesthetic into subarachnoid space
- Rapid onset (5-10 minutes)
- Dense motor and sensory block
- Duration: 1-6 hours
- Ideal for lower abdominal, pelvic, and lower extremity surgery
Epidural Anesthesia
- Local anesthetic into epidural space
- Slower onset (15-30 minutes)
- Titratable level of block
- Can be continuous via catheter
- Excellent for postoperative pain control
Peripheral Nerve Blocks
- Target specific nerve or nerve groups
- Ultrasound-guided placement
- Minimal systemic effects
- Excellent postoperative analgesia
- Examples: brachial plexus, femoral, sciatic blocks
Local Anesthesia
Local anesthesia involves the application or injection of anesthetic agents to a specific, localized area to block sensation while maintaining consciousness and normal physiologic function elsewhere in the body.
Techniques:
- Topical: Surface application of anesthetic
- Infiltration: Direct injection into tissues
- Field Block: Injection around surgical area
- Nerve Block: Injection near specific nerves
Applications:
- Minor surgical procedures
- Dermatologic procedures
- Dental procedures
- Wound repair and suturing
- Biopsy procedures
Monitored Anesthesia Care (MAC) / Sedation
Sedation involves the administration of medications to reduce anxiety, discomfort, and memory while maintaining the patient’s ability to respond purposefully to verbal or tactile stimulation.
Levels of Sedation
Minimal
Anxiolysis
Normal response to verbal stimulation
Moderate
Conscious sedation
Purposeful response to verbal/tactile
Deep
Deep sedation
Purposeful response to repeated stimulation
General
Anesthesia
Unresponsive to painful stimulation
Methods of Administration
Inhalational Administration
Inhalational anesthetics are volatile liquids or gases administered through the respiratory system. They provide controllable anesthesia with rapid onset and offset, making them ideal for maintaining general anesthesia during surgical procedures.
Mechanism:
- Alveolar uptake into bloodstream
- Distribution to brain via circulation
- Reversible binding to neuronal receptors
- Elimination through exhalation
- Concentration-dependent effects
Advantages:
- Rapid onset and recovery
- Precise control of anesthetic depth
- Minimal accumulation
- Non-dependent on organ function
- Real-time monitoring capability
Memory Aid: “DESI” for Volatile Agents
Desflurane – Fastest onset/offset
Enflurane – Rarely used (seizure risk)
Sevoflurane – Smooth induction, pleasant odor
Isoflurane – Standard maintenance agent
Intravenous Administration
Intravenous anesthetics provide rapid, precise drug delivery directly into the systemic circulation. This route offers immediate onset, predictable pharmacokinetics, and the ability to titrate effects in real-time.
Bolus Administration
- Rapid drug delivery
- Immediate onset of action
- Used for induction
- Risk of overdosing
- Requires careful dosing
Continuous Infusion
- Steady-state maintenance
- Precise control of depth
- Reduced drug accumulation
- Requires infusion pumps
- TIVA (Total IV Anesthesia)
Target-Controlled Infusion
- Computer-controlled delivery
- Pharmacokinetic modeling
- Predicted plasma/effect-site concentrations
- Enhanced precision
- Reduced learning curve
Regional Administration Techniques
Regional anesthesia techniques involve the precise placement of local anesthetics near nerve structures to provide anesthesia and analgesia to specific anatomical regions while preserving consciousness and systemic function.
Administration Process Flow
Patient Assessment
Anatomical Identification
Precise Injection
Guidance Methods:
- Anatomical landmarks: Traditional palpation-based technique
- Nerve stimulator: Electrical stimulation to locate nerves
- Ultrasound guidance: Real-time visualization of structures
- Fluoroscopic guidance: X-ray guidance for deep structures
Injection Considerations:
- Sterile technique maintenance
- Incremental injection with aspiration
- Patient communication throughout
- Monitoring for systemic toxicity
- Post-injection block assessment
Stages and Effects of Anesthesia
Guedel’s Classification Mnemonic: “AIDE”
A
Analgesia
Stage I
I
Initial Excitement
Stage II
D
Desired Surgical
Stage III
E
Emergency
Stage IV
Stage I: Analgesia (Conscious)
Clinical Characteristics:
- Patient remains conscious and conversant
- Progressive loss of pain sensation
- Maintained protective reflexes
- Normal breathing pattern
- Stable vital signs
- May experience euphoria or anxiety
Nursing Considerations:
- Provide reassurance and explanation
- Maintain patient dignity and privacy
- Monitor for signs of progression
- Prepare for next stage transition
- Continue baseline monitoring
- Assess pain relief effectiveness
Clinical Pearl: This stage is ideal for minor procedures and regional anesthesia supplementation. Patients can cooperate with positioning and provide feedback about comfort.
Stage II: Excitement/Delirium (Dangerous Stage)
Clinical Characteristics:
- Loss of consciousness begins
- Irregular breathing patterns
- Increased muscle tone and reflexes
- Possible laryngospasm or breath-holding
- Cardiovascular instability
- Involuntary movements and struggling
- Risk of vomiting and aspiration
Critical Nursing Actions:
- Ensure patient safety and restraint if needed
- Maintain airway patency
- Prepare suction equipment
- Monitor oxygen saturation continuously
- Assist anesthesiologist with rapid progression
- Have emergency medications ready
- Document all observations and interventions
⚠️ Critical Alert: This is the most dangerous stage of anesthesia. Modern techniques with IV induction and muscle relaxants aim to minimize time in this stage. Never leave the patient unattended.
Stage III: Surgical Anesthesia (Target Stage)
Plane 1 (Light):
- Regular breathing
- Pupils mobile, react to light
- Lid reflex present
- Suitable for superficial procedures
Plane 2 (Medium):
- Breathing regular, deeper
- Pupils begin to fix centrally
- Lid reflex absent
- Ideal for most procedures
Plane 3 (Deep):
- Pupils fixed and dilated
- Intercostal breathing begins
- Muscle relaxation complete
- Deep abdominal surgery
Optimal Nursing Management:
- Continuous vital sign monitoring
- Airway management support
- Temperature regulation
- Fluid balance monitoring
- Positioning and pressure point care
- Surgical site preparation assistance
- Equipment readiness for emergence
- Medication administration support
Stage IV: Medullary Depression (Overdose)
⚠️ LIFE-THREATENING STAGE – IMMEDIATE INTERVENTION REQUIRED
Clinical Signs:
- Respiratory depression or apnea
- Cardiovascular collapse
- Pupils widely dilated and fixed
- Absent reflexes
- Weak, thready pulse
- Hypotension and shock
Emergency Actions:
- Immediate cessation of anesthetic
- 100% oxygen ventilation
- IV fluid resuscitation
- Vasopressor support
- CPR if indicated
- Notify emergency team
Anesthesia Equipment & Monitoring
Anesthesia Machine Components
Gas Supply System
- • Central or cylinder supply
- • Pressure regulators
- • Flow meters
- • Safety relief valves
- • Oxygen failure alarm
Vaporizer System
- • Agent-specific vaporizers
- • Temperature compensation
- • Concentration dials
- • Interlock mechanisms
- • Agent monitoring
Breathing Circuit
- • Circle or non-rebreathing
- • CO₂ absorber
- • Unidirectional valves
- • Adjustable pressure valve
- • Reservoir bag
Ventilator
- • Volume/pressure control
- • PEEP adjustment
- • Respiratory rate setting
- • I:E ratio control
- • Disconnect alarm
Monitoring System
- • Gas concentration analysis
- • Airway pressure monitoring
- • Volume measurements
- • Capnography
- • Oxygen analyzer
Safety Features
- • Hypoxic guard
- • Pin index system
- • Scavenging system
- • Anti-hypoxia valve
- • Emergency oxygen flush
Patient Monitoring Standards
ASA Basic Monitoring Mnemonic: “OPEN HEARTS”
Oxygen concentration
Pulse oximetry
ECG
NIBP (Non-invasive BP)
Halothane (agent monitoring)
ETCO₂ (Capnography)
Airway pressure
Respiratory volume
Temperature
Stethoscope
Standard Monitoring (ASA Basic):
Cardiovascular
- • Continuous ECG
- • Blood pressure (NIBP)
- • Pulse oximetry
Respiratory
- • Continuous capnography
- • Inspired oxygen concentration
- • Airway pressure monitoring
Other
- • Temperature monitoring
- • Neuromuscular monitoring
- • Agent concentration
Enhanced Monitoring (High-Risk Cases):
Invasive Cardiovascular
- • Arterial line (continuous BP)
- • Central venous pressure
- • Pulmonary artery catheter
- • Transesophageal echocardiography
Neurological
- • Bispectral index (BIS)
- • Cerebral oximetry
- • Intracranial pressure
- • Evoked potentials
Specialized
- • Urine output monitoring
- • Blood gas analysis
- • Coagulation monitoring
- • Cardiac output monitoring
Airway Management Equipment
Face Masks
- • Various sizes (0-6)
- • Transparent material
- • Cushioned seal
- • Low dead space
Laryngeal Mask Airways
- • Supraglottic airway device
- • Sizes 1-6
- • Inflatable cuff
- • Easy insertion
Endotracheal Tubes
- • Cuffed and uncuffed
- • Various sizes (2.5-10mm)
- • Single and double lumen
- • Murphy eye design
Laryngoscopes
- • Miller (straight) blades
- • Macintosh (curved) blades
- • Fiber-optic scopes
- • Video laryngoscopes
Anesthetic Drugs
Intravenous Anesthetics
IV Induction Agents
| Drug | Dose (mg/kg) | Onset | Duration | Key Features |
|---|---|---|---|---|
| Propofol | 2-2.5 | 30-60 sec | 5-10 min | Smooth induction/emergence, antiemetic properties |
| Etomidate | 0.2-0.3 | 30-60 sec | 3-5 min | Cardiovascular stability, myoclonus risk |
| Ketamine | 1-2 | 1-2 min | 15-30 min | Dissociative anesthesia, bronchodilation |
| Thiopental | 3-5 | 30-40 sec | 5-10 min | Cerebral protection, cardiovascular depression |
IV Anesthetic Memory Aid: “KEPT”
Ketamine – Keeps BP up (sympathomimetic)
Etomidate – Excellent for unstable patients
Propofol – Popular choice, smooth emergence
Thiopental – Traditional barbiturate
Volatile Anesthetics
Inhaled Anesthetic Agents
| Agent | MAC (%) | Blood:Gas | Characteristics | Clinical Use |
|---|---|---|---|---|
| Sevoflurane | 2.0 | 0.65 | Pleasant odor, non-irritating | Ideal for mask induction, pediatrics |
| Desflurane | 6.0 | 0.42 | Fastest onset/offset | Long procedures, rapid emergence |
| Isoflurane | 1.15 | 1.4 | Stable, cost-effective | Maintenance anesthesia standard |
| Nitrous Oxide | 105 | 0.47 | Analgesic, rapid onset/offset | Adjunct to other agents |
MAC (Minimum Alveolar Concentration) Concept:
MAC is the alveolar concentration of anesthetic at which 50% of patients will not move in response to surgical incision. It’s the ED₅₀ for anesthetic potency and is used to compare different agents.
Neuromuscular Blocking Agents
Depolarizing Relaxant
Succinylcholine (Suxamethonium)
- Dose: 1-1.5 mg/kg IV
- Onset: 30-60 seconds
- Duration: 5-10 minutes
- Metabolism: Plasma cholinesterases
- Use: Rapid sequence intubation
Contraindications:
- • Hyperkalemia risk patients
- • Malignant hyperthermia susceptibility
- • Neuromuscular diseases
- • Recent burns or trauma
Non-Depolarizing Relaxants
Rocuronium
Onset: 1-2 min, Duration: 30-60 min, Reversal: Sugammadex
Vecuronium
Onset: 2-3 min, Duration: 30-45 min, Reversal: Neostigmine
Atracurium
Onset: 2-3 min, Duration: 20-40 min, Reversal: Neostigmine
Cisatracurium
Onset: 2-3 min, Duration: 25-45 min, Organ-independent
Muscle Relaxant Reversal: “SANE”
Sugammadex – for rocuronium/vecuronium
Atropine – with neostigmine (anticholinergic)
Neostigmine – for non-depolarizing agents
Edrophonium – short-acting alternative
Opioid Analgesics
Ultra-Short Acting
Remifentanil
- • Context-sensitive half-life: 3-4 min
- • Ester metabolism
- • Organ-independent clearance
- • Infusion-based dosing
Short Acting
Fentanyl
- • 50-100x more potent than morphine
- • Duration: 30-60 minutes
- • Minimal histamine release
- • Cardiovascular stability
Intermediate Acting
Morphine
- • Gold standard opioid
- • Duration: 2-4 hours
- • Active metabolites
- • Excellent postop analgesia
Opioid Side Effects Management:
- Respiratory depression: Monitor, naloxone if severe
- Nausea/vomiting: Antiemetics, multimodal approach
- Pruritus: Antihistamines, low-dose naloxone
- Constipation: Prophylactic bowel regimen
- Sedation: Dose reduction, stimulants if needed
- Tolerance: Rotation, multimodal analgesia
Nursing Implementation in Anesthesia Care
Preoperative Nursing Care
Assessment Priorities:
Airway Assessment
- • Mallampati classification
- • Thyromental distance
- • Neck mobility and extension
- • Previous difficult intubation history
- • Dental examination
Cardiovascular Status
- • Exercise tolerance assessment
- • Recent cardiac events
- • Current medications
- • Baseline vital signs
- • ECG abnormalities
Respiratory Function
- • Smoking history and cessation
- • Asthma or COPD status
- • Recent respiratory infections
- • Sleep apnea screening
- • Baseline oxygen saturation
Preparation Activities:
Documentation Review
- • Verify consent forms completion
- • Check allergy documentation
- • Review medication reconciliation
- • Confirm NPO status
- • Validate procedure details
Physical Preparation
- • Remove jewelry, makeup, nail polish
- • Ensure proper attire
- • Insert IV access
- • Administer premedications
- • Perform site marking if required
Patient Education
- • Explain anesthetic plan
- • Discuss postoperative expectations
- • Address anxiety and concerns
- • Review pain management options
- • Provide family communication plan
Intraoperative Nursing Care
Intraoperative Workflow
Patient Arrival
Positioning & Monitoring
Continuous Assessment
Safety Priorities
- • Time-out procedure verification
- • Patient identification confirmation
- • Surgical site verification
- • Equipment safety checks
- • Fire safety precautions
- • Electrical safety monitoring
- • Positioning safety assessment
Monitoring Responsibilities
- • Continuous vital sign monitoring
- • Anesthetic depth assessment
- • Fluid balance tracking
- • Temperature management
- • Neuromuscular monitoring
- • Blood loss estimation
- • Urine output monitoring
Intervention Priorities
- • Medication administration support
- • Airway management assistance
- • IV access maintenance
- • Equipment troubleshooting
- • Emergency response readiness
- • Communication with team
- • Documentation accuracy
Intraoperative Nursing Priorities: “SAFE CARE”
Safety first – patient and team
Airway management support
Fluid balance monitoring
Emergency preparedness
Communication with team
Anesthesia depth monitoring
Respiratory status assessment
Equipment function verification
Postoperative/Recovery Nursing Care
Immediate Recovery (PACU):
Respiratory Assessment
- • Airway patency verification
- • Oxygen saturation monitoring
- • Respiratory rate and quality
- • Breath sound assessment
- • Signs of respiratory depression
Cardiovascular Monitoring
- • Blood pressure stability
- • Heart rate and rhythm
- • Perfusion indicators
- • Fluid balance status
- • Signs of bleeding
Neurological Assessment
- • Level of consciousness
- • Orientation status
- • Motor function return
- • Sensory function assessment
- • Pain level evaluation
Recovery Interventions:
Pain Management
- • Regular pain assessments
- • Multimodal analgesic approach
- • Non-pharmacologic interventions
- • Side effect monitoring
- • Patient education on pain control
Complication Prevention
- • Nausea/vomiting management
- • Hypothermia prevention
- • DVT prophylaxis
- • Wound care monitoring
- • Infection prevention measures
Discharge Preparation
- • Recovery criteria assessment
- • Home care instructions
- • Follow-up appointments
- • Emergency contact information
- • Medication reconciliation
PACU Discharge Criteria (Modified Aldrete Score):
Move 4 extremities: 2
Move 2 extremities: 1
Unable to move: 0
Breathes deeply: 2
Dyspnea/shallow: 1
Apneic: 0
BP ±20% baseline: 2
BP ±20-50%: 1
BP ±50%: 0
Fully awake: 2
Arousable: 1
Not responding: 0
>92% on room air: 2
>90% on O₂: 1
<90% with O₂: 0
Minimum score for discharge: 8/10
Special Population Considerations
Pediatric Patients:
- • Age-appropriate communication and comfort measures
- • Parental presence during induction when appropriate
- • Weight-based medication calculations
- • Temperature regulation critical
- • Faster onset/offset of volatile agents
- • Higher oxygen consumption rates
- • Careful fluid management
- • PONV prevention strategies
Geriatric Patients:
- • Reduced drug clearance and prolonged effects
- • Increased sensitivity to anesthetic agents
- • Careful positioning due to fragile skin
- • Cognitive assessment for delirium
- • Polypharmacy interaction considerations
- • Slower recovery and mobilization
- • Enhanced hypothermia risk
- • Frequent comorbidity management
Obese Patients:
- • Difficult airway management anticipation
- • Dosing based on ideal vs. actual weight
- • Positioning challenges and pressure point care
- • Sleep apnea screening and management
- • Extended recovery time expectations
- • DVT prophylaxis importance
- • Respiratory function monitoring
- • Equipment weight limits consideration
Pregnant Patients:
- • Fetal monitoring during procedures
- • Left uterine displacement positioning
- • Aspiration risk prevention
- • Teratogenic drug avoidance
- • Aortocaval compression awareness
- • Physiologic changes accommodation
- • Emergency cesarean preparation
- • Neonatal resuscitation readiness
Complications & Emergency Management
Respiratory Complications
Laryngospasm
Signs & Symptoms:
- • Complete or partial airway obstruction
- • Stridor or absent breath sounds
- • Chest wall retraction
- • Rapid desaturation
- • Paradoxical chest movement
Management:
- • Remove irritating stimulus
- • 100% oxygen with positive pressure
- • Deepen anesthesia (propofol 0.5-1 mg/kg)
- • Succinylcholine 0.1-0.5 mg/kg if severe
- • Consider CPAP 5-10 cmH₂O
Bronchospasm
Signs & Symptoms:
- • Wheezing on expiration
- • Increased peak airway pressures
- • Prolonged expiratory phase
- • Decreased tidal volumes
- • Hypercapnia
Management:
- • Deepen anesthesia
- • Salbutamol 2-8 puffs via ETT
- • Consider ketamine 0.5-1 mg/kg
- • Magnesium 1-2g IV if severe
- • Rule out pneumothorax/aspiration
Aspiration
Risk Factors:
- • Recent oral intake
- • Pregnancy, obesity
- • Emergency surgery
- • Gastroesophageal reflux
- • Altered consciousness
Management:
- • Head-down, lateral positioning
- • Immediate suction of airway
- • Bronchoscopy if large particles
- • PEEP and lung-protective ventilation
- • Avoid steroids, antibiotics unless indicated
Pneumothorax
Signs & Symptoms:
- • Sudden increase in airway pressure
- • Decreased breath sounds
- • Hypotension and tachycardia
- • Decreased compliance
- • Shifted heart sounds
Management:
- • Immediate chest decompression if tension
- • 100% oxygen administration
- • Chest tube insertion
- • Hemodynamic support as needed
- • Chest X-ray confirmation
Cardiovascular Complications
Hypotension
Common Causes:
- • Anesthetic overdose
- • Hypovolemia/bleeding
- • Myocardial depression
- • Vasodilation
- • Arrhythmias
Management:
- • Reduce anesthetic depth
- • IV fluid bolus 10-20 ml/kg
- • Ephedrine 5-10mg or phenylephrine 100-200mcg
- • Check for bleeding
- • Consider inotropic support
Hypertension
Common Causes:
- • Inadequate analgesia
- • Light anesthesia
- • Hypercapnia/hypoxia
- • Drug interactions
- • Fluid overload
Management:
- • Deepen anesthesia
- • Increase opioid analgesia
- • Labetalol 5-20mg IV
- • Esmolol 0.5-1mg/kg
- • Check ventilation adequacy
Arrhythmias
Common Types:
- • Bradycardia
- • Tachycardia
- • Atrial fibrillation
- • Ventricular ectopy
- • Heart block
Management:
- • Identify and treat cause
- • Atropine 0.5-1mg for bradycardia
- • Beta-blockers for tachycardia
- • Correct electrolyte abnormalities
- • ACLS protocols if unstable
Life-Threatening Anesthetic Emergencies
Malignant Hyperthermia (MH)
Early Signs:
- • Unexplained tachycardia
- • Increased ETCO₂ (>55 mmHg)
- • Masseter muscle rigidity
- • Increased oxygen consumption
- • Metabolic and respiratory acidosis
Late Signs:
- • Hyperthermia (>38.8°C)
- • Generalized muscle rigidity
- • Hyperkalemia, hypercalcemia
- • Myoglobinuria (cola-colored urine)
- • Cardiac arrhythmias
Emergency Treatment:
- 1. Discontinue triggering agents immediately
- 2. Dantrolene 2.5 mg/kg IV bolus, repeat PRN
- 3. Hyperventilate with 100% O₂
- 4. Cool patient (ice, cold saline)
- 5. Treat hyperkalemia and acidosis
- 6. Monitor urine output and CK levels
Anaphylaxis
Clinical Signs:
- • Cardiovascular collapse
- • Bronchospasm and hypoxia
- • Urticaria and angioedema
- • Increased airway pressures
- • Unexplained hypotension
Common Triggers:
- • Neuromuscular blocking agents
- • Antibiotics (penicillins, cephalosporins)
- • Latex exposure
- • Chlorhexidine
- • Blood products
Emergency Treatment:
- 1. Epinephrine 10-100 mcg IV (0.1-1 mL of 1:10,000)
- 2. Remove/discontinue triggering agent
- 3. 100% oxygen, support airway
- 4. IV fluid resuscitation 20-50 mL/kg
- 5. Hydrocortisone 200mg + H₁/H₂ blockers
- 6. Bronchodilators if needed
Emergency Response Mnemonic: “ABCDE”
A
Airway
Ensure patency
B
Breathing
Ventilation support
C
Circulation
Hemodynamic support
D
Disability
Neurological assessment
E
Exposure
Environment control
Key Takeaways for Nursing Practice
Essential Knowledge Points:
- Understanding the four stages of anesthesia and their clinical implications is crucial for safe patient care
- Different anesthetic types (general, regional, local) have specific indications and nursing considerations
- Comprehensive patient assessment is fundamental to preventing complications
- Emergency recognition and response skills can be life-saving
- Continuous monitoring and documentation are essential throughout the perioperative period
Professional Development:
- Stay current with evidence-based anesthesia practices and guidelines
- Develop strong communication skills for interprofessional collaboration
- Consider specialization in perioperative or critical care nursing
- Pursue continuing education in anesthesia-related topics
- Participate in simulation training for emergency scenarios
Final Thoughts
Anesthesia nursing requires a comprehensive understanding of pharmacology, physiology, and emergency management. Your role in ensuring patient safety throughout the perioperative period is invaluable. Continue to build your knowledge base, develop critical thinking skills, and always prioritize patient-centered care.
References & Further Reading
1. Miller, R. D., et al. (2020). Miller’s Anesthesia (9th ed.). Elsevier.
2. American Society of Anesthesiologists. (2020). Standards for Basic Anesthetic Monitoring.
3. Butterworth, J. F., et al. (2018). Morgan & Mikhail’s Clinical Anesthesiology (6th ed.). McGraw-Hill.
4. Association of periOperative Registered Nurses. (2021). Guidelines for Perioperative Practice.
5. Nagelhout, J. J., & Elisha, S. (2018). Nurse Anesthesia (6th ed.). Elsevier.
6. Malignant Hyperthermia Association of the United States. (2020). Emergency Treatment Protocol.
Note: This educational material is designed for nursing students and should be used in conjunction with clinical instruction and current institutional protocols. Always refer to your facility’s policies and consult with experienced practitioners when caring for patients.