
Oral Cavity Disorders
Lips, Gums, and Teeth Conditions
Comprehensive Nursing Study Guide
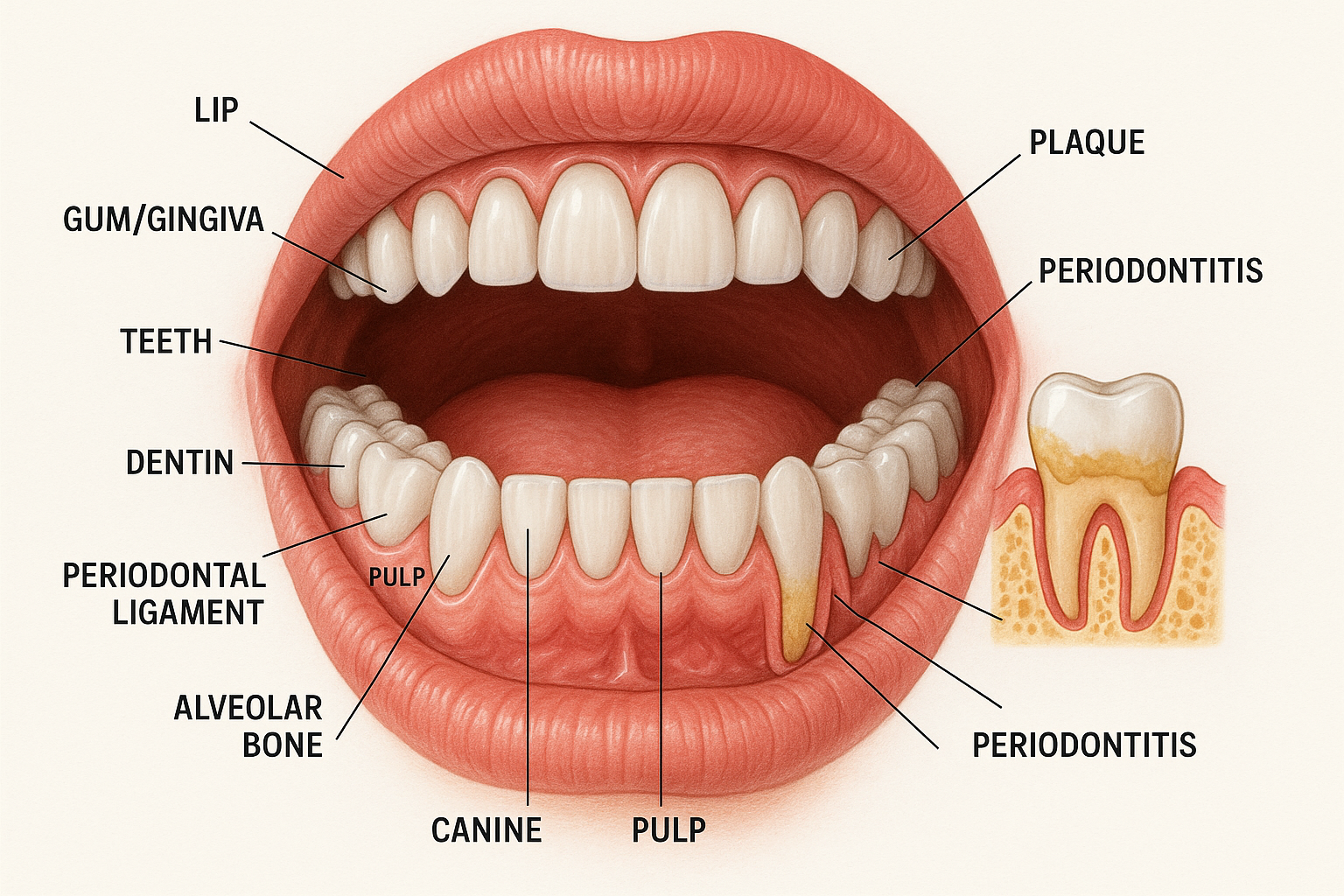
Figure 1: Comprehensive oral cavity anatomy showing normal and pathological conditions
1. Oral Cavity Anatomy Review
Essential Anatomical Structures
Lips (Labia)
- • Vermillion border (red margin)
- • Wet mucosa (inner surface)
- • Labial frenum (upper & lower)
- • Orbicularis oris muscle
Gums (Gingiva)
- • Free gingiva (gum margin)
- • Attached gingiva
- • Gingival sulcus (0.5-3mm normal)
- • Interdental papilla
Teeth Structure
- • Enamel (outer protective layer)
- • Dentin (middle layer)
- • Pulp (innermost, contains nerves)
- • Cementum (root surface)
Memory Aid: Tooth Layers (Outside to Inside)
“Every Dentist Practices Carefully”
- Enamel – Hardest substance in body
- Dentin – Majority of tooth structure
- Pulp – Contains blood vessels and nerves
- Cementum – Covers tooth root
Normal Gingival Health Indicators
2. Nursing Assessment Framework
Visual Inspection
- Color: Pink (normal), red (inflammation), white (infection/trauma)
- Swelling: Localized vs. generalized edema
- Texture: Smooth, rough, ulcerated, or nodular
- Moisture: Adequate saliva vs. xerostomia
- Lesions: Size, shape, borders, distribution
Palpation Assessment
- Temperature: Normal vs. increased heat
- Consistency: Firm, soft, fluctuant, or indurated
- Mobility: Fixed vs. mobile masses
- Tenderness: Pain response to gentle pressure
- Lymph nodes: Submandibular, cervical chain
Assessment Mnemonic: “ORAL HEALTH”
Odor – Halitosis present?
Redness – Inflammation signs?
Asymmetry – Unilateral changes?
Lesions – Ulcers, growths?
Heat – Temperature changes?
Edema – Swelling present?
Adhesion – Mobility issues?
Tenderness – Pain on palpation?
Hydration – Moisture adequate?
3. Lip Disorders
Cheilitis (Lip Inflammation)
Pathophysiology
Inflammation of lip tissues caused by environmental factors, allergens, infections, or nutritional deficiencies. Results in compromised barrier function and increased susceptibility to secondary infections.
Types & Causes
- Contact Cheilitis: Cosmetics, toothpaste, foods
- Actinic Cheilitis: Sun exposure (precancerous)
- Angular Cheilitis: Candida, vitamin B deficiency
- Eczematous Cheilitis: Atopic dermatitis
- Infectious Cheilitis: Herpes simplex, bacterial
Clinical Presentation
- • Dry, cracked, or peeling lips
- • Erythema and edema
- • Pain, burning, or itching
- • Fissures at lip corners (angular)
- • Secondary bacterial infection possible
Herpes Simplex Labialis (Cold Sores)
Pathophysiology
Caused by HSV-1 (occasionally HSV-2). Initial infection establishes latency in trigeminal ganglia. Reactivation triggered by stress, illness, immunosuppression, or UV exposure. Viral replication causes vesicle formation and tissue destruction.
Disease Progression
Clinical Pearl
Antiviral therapy (acyclovir, valacyclovir) is most effective when started during prodromal phase. Topical anesthetics can provide symptomatic relief. Emphasize infection control – HSV is highly contagious during active lesions.
Nursing Interventions for Lip Disorders
Immediate Care
- • Apply lip balm with SPF 15+ regularly
- • Avoid licking or picking at lesions
- • Use gentle, fragrance-free cleansers
- • Apply cool compresses for comfort
Long-term Management
- • Identify and avoid triggers
- • Maintain adequate hydration
- • Use humidifier in dry environments
- • Monitor for secondary infections
4. Gum (Periodontal) Disorders
Gingivitis
Pathophysiology
Reversible inflammatory response to bacterial plaque accumulation along gum line. Plaque biofilm contains gram-positive and gram-negative bacteria producing toxins that trigger inflammatory cascade. Increased vascular permeability leads to edema, erythema, and bleeding tendency.
Risk Factors
- • Poor oral hygiene
- • Hormonal changes
- • Diabetes mellitus
- • Smoking/tobacco use
- • Certain medications
- • Immunocompromised state
Clinical Signs
- • Red, swollen gums
- • Bleeding on brushing/flossing
- • Tender to touch
- • Halitosis (bad breath)
- • Normal sulcus depth (<3mm)
- • No bone loss on X-ray
Management
- • Improve oral hygiene
- • Professional cleaning
- • Antimicrobial rinse
- • Address systemic factors
- • Regular dental follow-up
- • Patient education
Periodontitis
Pathophysiology
Progressive destruction of periodontal ligament and alveolar bone due to chronic bacterial infection. Host immune response becomes destructive, with inflammatory mediators causing tissue breakdown. Irreversible process leading to tooth mobility and potential loss.
Red Flag: Systemic Complications
Periodontitis is linked to cardiovascular disease, diabetes complications, respiratory infections, and adverse pregnancy outcomes. Chronic inflammation and bacteremia contribute to systemic disease progression.
Periodontitis Progression
Mild
3-4mm pockets
Slight bone loss
Moderate
4-6mm pockets
Moderate bone loss
Severe
>6mm pockets
Significant bone loss
Advanced
Tooth mobility
Potential extraction
Acute Necrotizing Ulcerative Gingivitis (ANUG)
Pathophysiology
Acute bacterial infection involving spirochetes and gram-negative anaerobes. Tissue necrosis occurs due to bacterial toxins and compromised host defense. Often associated with stress, immunosuppression, poor nutrition, and smoking.
Clinical Pearl: “Trench Mouth”
Classical triad: 1) Painful bleeding gums, 2) Ulceration with pseudomembrane, 3) Fetid breath odor. May present with fever and malaise. Requires immediate antimicrobial therapy (metronidazole or penicillin).
Periodontal Disease Mnemonic: “GUMS HURT”
Gingivitis (early stage)
Ulceration (ANUG)
Mobility (advanced disease)
Support loss (bone destruction)
Halitosis (bad breath)
Uncontrolled diabetes (risk factor)
Recession (gum retreat)
Tobacco use (major risk)
5. Tooth Disorders
Dental Caries (Tooth Decay)
Pathophysiology
Multifactorial disease involving bacterial acid production (primarily S. mutans), fermentable carbohydrates, susceptible tooth surface, and time. Bacterial metabolism produces lactic acid, lowering pH and demineralizing enamel. Progressive destruction through enamel → dentin → pulp.
Caries Classification by Depth
Class I
Enamel only
White spot lesion
Reversible
Class II
Into dentin
Visible cavity
Requires filling
Class III
Near pulp
Severe pain
May need root canal
Class IV
Pulp involved
Abscess risk
Extraction possible
Risk Factors
- Dietary: Frequent sugar/acid exposure
- Bacterial: High S. mutans colonization
- Salivary: Reduced flow, low pH buffering
- Fluoride: Inadequate exposure
- Host: Deep fissures, crowding
- Behavioral: Poor oral hygiene
Clinical Progression
- Early: Asymptomatic, white spots
- Enamel: Sensitivity to sweets
- Dentin: Temperature sensitivity
- Pulp: Spontaneous pain, throbbing
- Periapical: Abscess formation
- Complications: Cellulitis, osteomyelitis
Pulpitis
Pathophysiology
Inflammation of dental pulp due to bacterial invasion, trauma, or chemical irritation. Confined space leads to increased pressure, compromised blood flow, and intense pain. May progress to pulp necrosis and periapical pathology.
Reversible Pulpitis
- Pain: Sharp, brief, stimulus-provoked
- Duration: Seconds after stimulus removal
- Triggers: Cold, sweet, acidic foods
- Treatment: Remove irritant, restoration
- Prognosis: Pulp can recover function
Irreversible Pulpitis
- Pain: Spontaneous, throbbing, severe
- Duration: Persists after stimulus removal
- Triggers: Heat more than cold
- Treatment: Root canal or extraction
- Prognosis: Pulp cannot recover
Dental Abscess
Pathophysiology
Localized collection of pus resulting from bacterial infection of necrotic pulp tissue. Infection spreads through apical foramen into periapical tissues. May progress to cellulitis, osteomyelitis, or systemic sepsis if untreated.
Emergency Signs – Refer Immediately
- • Fever >101°F (38.3°C)
- • Facial swelling extending beyond local area
- • Difficulty swallowing or breathing
- • Trismus (difficulty opening mouth)
- • Signs of Ludwig’s angina or necrotizing fasciitis
Clinical Pearl: Pain Assessment
Apical abscess: Constant, throbbing pain worse with biting. Tooth feels “high” or extruded. Periodontal abscess: Localized gum swelling, drainage possible. May have less severe pain than apical abscess.
Tooth Pain Assessment: “PQRST Method”
Provocation – What triggers the pain?
Quality – Sharp, dull, throbbing, burning?
Radiation – Does pain spread elsewhere?
Severity – Pain scale 1-10
Timing – Constant, intermittent, duration?
6. Nursing Interventions
Pain Management
Pharmacological
- • NSAIDs: Ibuprofen 600-800mg q6-8h (anti-inflammatory)
- • Acetaminophen: 650-1000mg q6h (analgesic)
- • Topical anesthetics: Benzocaine, lidocaine gels
- • Antibiotics: If systemic signs present
Non-pharmacological
- • Cold compress: 15-20min q2-3h for acute swelling
- • Warm saltwater rinses: ½ tsp salt in 8oz warm water
- • Avoid extreme temperatures in food/drink
- • Elevate head when sleeping
Infection Control
Standard Precautions
- • Hand hygiene before/after oral care
- • Gloves for all oral cavity contact
- • Eye protection if splashing risk
- • Proper disposal of contaminated materials
Patient Isolation
- • Contact precautions for MRSA oral infections
- • Droplet precautions for respiratory pathogens
- • Private room if immunocompromised
- • Education on transmission prevention
Oral Hygiene Protocol for Hospitalized Patients
Frequency
- • Conscious patients: q12h minimum
- • Unconscious/ventilated: q6-8h
- • Post-oral surgery: q2-4h
- • Immunocompromised: q4-6h
Technique
- • 45° angle toothbrush placement
- • Gentle circular motions
- • 2-minute duration minimum
- • Include tongue cleaning
Products
- • Soft-bristled toothbrush
- • Fluoride toothpaste
- • Chlorhexidine rinse (0.12%)
- • Suction toothbrush if indicated
Documentation Requirements
Document oral assessment findings, interventions performed, patient response, and any complications. Include pain scores, infection signs, medication administration, and referrals made. Use standardized oral assessment tools when available.
7. Patient Education
Preventive Care Education
Daily Oral Hygiene
- • Brush twice daily with fluoride toothpaste
- • Use proper brushing technique (2 minutes)
- • Floss daily to remove plaque between teeth
- • Rinse with antimicrobial mouthwash
- • Replace toothbrush every 3-4 months
Dietary Modifications
- • Limit sugary and acidic foods/drinks
- • Avoid frequent snacking
- • Drink water after meals
- • Chew sugar-free gum to stimulate saliva
- • Include calcium and vitamin D rich foods
Professional Care Schedule
Routine Visits
- • Dental checkup every 6 months
- • Professional cleaning as recommended
- • Fluoride treatments for high-risk patients
- • Dental X-rays per provider guidelines
- • Oral cancer screening annually
Special Populations
- • Diabetes: More frequent cleanings
- • Pregnancy: Dental visit each trimester
- • Elderly: Modified techniques, more frequent visits
- • Immunocompromised: Prophylactic care
- • Smokers: Cessation counseling, frequent monitoring
Patient Education Mnemonic: “SMILE BRIGHT”
Sugar reduction in diet
Mouthwash use daily
Immediate care for problems
Limit acidic beverages
Every 6 months dental visit
Brush twice daily properly
Replace toothbrush regularly
Increase water intake
Gum disease prevention focus
Halt tobacco use completely
Tongue cleaning important
When to Seek Immediate Care
Urgent Situations
- • Severe, persistent tooth pain
- • Facial swelling or fever
- • Trauma with tooth loss/fracture
- • Uncontrolled bleeding from gums
- • Signs of oral infection spreading
Monitoring Required
- • Persistent bad breath despite good hygiene
- • Changes in taste or sensation
- • White or red patches in mouth
- • Loose teeth or bite changes
- • Jaw pain or clicking
8. Complications & Red Flags
Life-Threatening Complications
Ludwig’s Angina
- • Bilateral neck swelling
- • “Hot potato” voice
- • Drooling, difficulty swallowing
- • Potential airway obstruction
- Action: Immediate ENT/surgery consult
Necrotizing Fasciitis
- • Rapid spreading facial infection
- • Skin color changes, crepitus
- • Severe systemic toxicity
- • High mortality if delayed treatment
- Action: Emergency surgical debridement
Systemic Complications
Cardiovascular
- • Bacterial endocarditis
- • Atherosclerosis progression
- • Increased MI/stroke risk
- • Hypertension exacerbation
Respiratory
- • Aspiration pneumonia
- • COPD exacerbations
- • Lung abscess formation
- • Ventilator-associated pneumonia
Metabolic
- • Diabetic complications
- • Glycemic control difficulties
- • Delayed wound healing
- • Increased infection risk
Escalation Decision Tree
Routine Care
• Localized, mild symptoms
• No systemic signs
• Patient stable
Provider Notification
• Moderate symptoms
• Fever present
• Pain uncontrolled
Emergency Response
• Airway compromise
• Rapid spreading
• Sepsis signs
Critical Assessment Points
Always assess airway patency in patients with facial swelling. Monitor for signs of sepsis in dental infections. Consider endocarditis risk in patients with valvular disease. Document progression of swelling with measurements and photos if possible.
Red Flag Assessment: “DANGER MOUTH”
Dysphagia (difficulty swallowing)
Airway compromise signs
Neck swelling bilateral
Generalized facial edema
Elevated temperature (>101°F)
Mental status changes
Oral breathing difficulty
Uncontrolled pain despite medication
Tachycardia, hypotension
High-risk patient (immunocompromised)
Key Takeaways for Nursing Practice
Assessment Priorities
- • Systematic oral cavity examination using ORAL HEALTH mnemonic
- • Early recognition of infection progression signs
- • Pain assessment using PQRST method
- • Risk factor identification and modification
Intervention Focus
- • Evidence-based oral hygiene protocols
- • Appropriate pain and infection management
- • Patient education emphasizing prevention
- • Timely recognition of complications requiring referral