
Acute Respiratory Distress Syndrome
Comprehensive Nursing Study Guide for ARDS Management and Care
Table of Contents
Definition and Overview
Acute Respiratory Distress Syndrome (ARDS) is a life-threatening condition characterized by rapid onset of widespread inflammation in the lungs, leading to severe hypoxemia and bilateral pulmonary infiltrates not fully explained by cardiac failure or fluid overload.
Key Characteristics
- Acute onset within 1 week of clinical insult
- Bilateral opacities on chest imaging
- Severe impairment of oxygenation
- Non-cardiogenic pulmonary edema
Epidemiology
- Incidence: 58.7 per 100,000 person-years
- Mortality rate: 35-46%
- ICU admission: 10% of all admissions
- Mechanical ventilation: 23% of cases
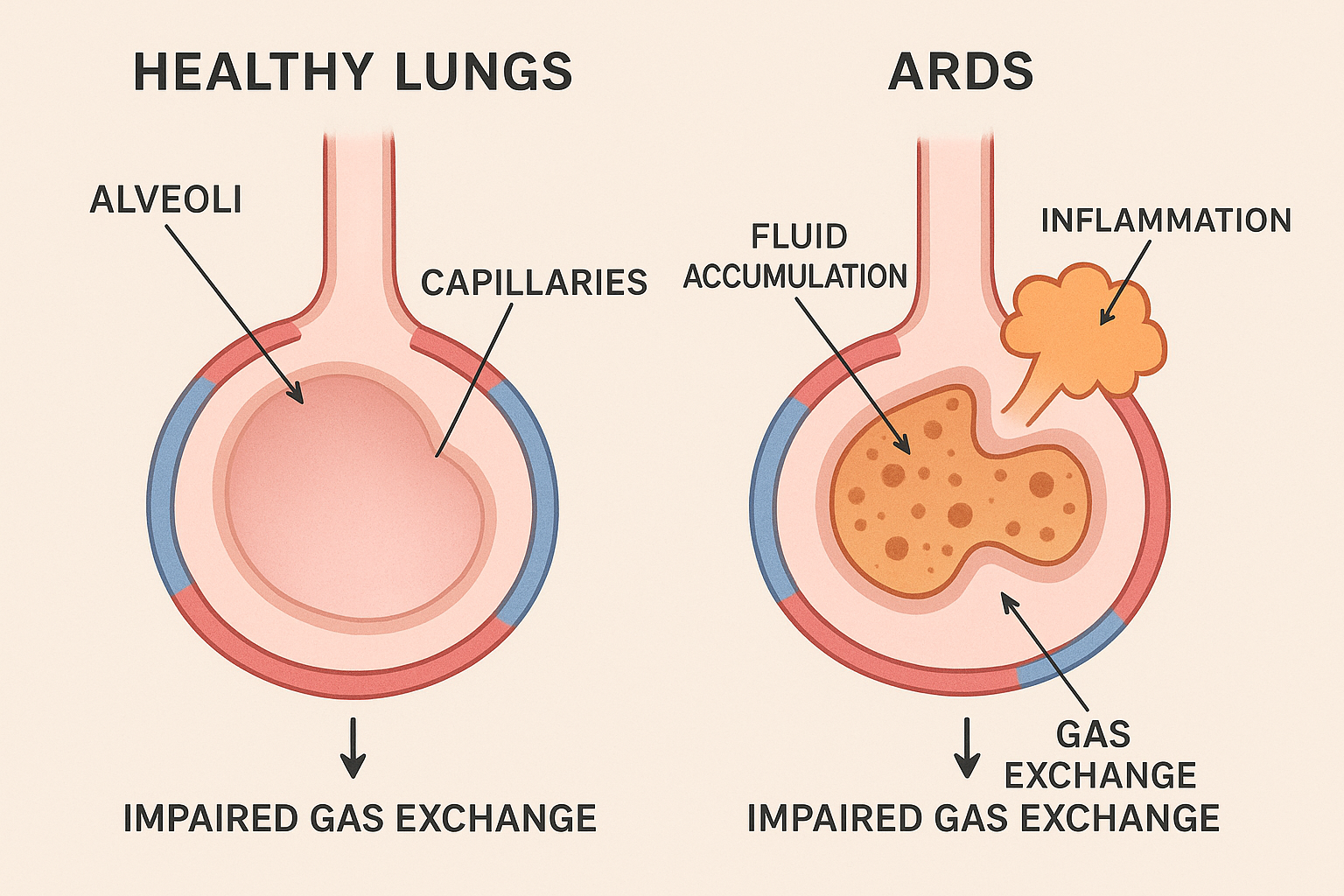
Pathophysiology
Memory Aid: “FLUID”
- Fluid accumulates in alveoli
- Lung inflammation and injury
- Uniform bilateral infiltrates
- Impaired gas exchange
- Decreased lung compliance
Phase 1: Exudative
- • Alveolar-capillary barrier damage
- • Protein-rich fluid leakage
- • Inflammatory cell infiltration
- • Surfactant dysfunction
- • Duration: 0-7 days
Phase 2: Proliferative
- • Fibroblast proliferation
- • Type II pneumocyte hyperplasia
- • Collagen deposition
- • Persistent inflammation
- • Duration: 7-21 days
Phase 3: Fibrotic
- • Extensive fibrosis
- • Alveolar remodeling
- • Reduced lung compliance
- • Impaired gas exchange
- • Duration: >21 days
Molecular Mechanisms
The pathogenesis of ARDS involves complex interactions between inflammatory mediators, cellular dysfunction, and mechanical stress. Initial injury triggers neutrophil activation, releasing inflammatory cytokines including tumor necrosis factor-alpha, interleukin-1, and interleukin-6.
This cascade leads to increased vascular permeability, surfactant dysfunction, and pulmonary vasoconstriction, ultimately resulting in the characteristic ventilation-perfusion mismatch seen in ARDS patients.
Causes and Risk Factors
Direct Lung Injury
| Cause | Frequency |
|---|---|
| Pneumonia | 46% |
| Aspiration | 7% |
| Pulmonary contusion | 17% |
| Inhalation injury | 2% |
| Near drowning | 0.5% |
Indirect Lung Injury
| Cause | Frequency |
|---|---|
| Sepsis | 36% |
| Trauma | 25% |
| Pancreatitis | 4% |
| Massive transfusion | 1% |
| Drug overdose | 1% |
High-Risk Populations
Age-Related
- • Age >65 years
- • Pediatric patients
- • Immunocompromised
Comorbidities
- • Chronic lung disease
- • Liver cirrhosis
- • Diabetes mellitus
Lifestyle Factors
- • Alcohol abuse
- • Smoking history
- • Malnutrition
Clinical Manifestations
Memory Aid: “SHARP”
Shortness of breath
Hypoxemia
Anxiety/Agitation
Restlessness
Pink frothy sputum
Respiratory System
- Severe dyspnea
- Tachypnea (>30 breaths/min)
- Use of accessory muscles
- Bilateral crackles
- Decreased breath sounds
- Intercostal retractions
Cardiovascular System
- Tachycardia
- Hypotension
- Arrhythmias
- Elevated central venous pressure
- Peripheral edema
- Decreased cardiac output
Neurological System
- Altered mental status
- Confusion
- Agitation
- Decreased level of consciousness
- Cyanosis
- Fatigue
Progressive Clinical Course
ARDS typically develops within 6-72 hours of the initial insult. Early recognition is crucial as the condition can rapidly progress from mild respiratory distress to severe hypoxemic respiratory failure requiring mechanical ventilation. The clinical presentation may vary depending on the underlying cause and patient comorbidities.
Diagnostic Criteria (Berlin Definition)
Berlin Definition (2012) – Current Standard
The Berlin Definition replaced the American-European Consensus Conference definition and provides more precise criteria for diagnosing ARDS with improved prognostic accuracy.
| Criteria | Mild ARDS | Moderate ARDS | Severe ARDS |
|---|---|---|---|
| Timing | Within 1 week of clinical insult or new/worsening respiratory symptoms | ||
| Chest Imaging | Bilateral opacities not fully explained by effusions, lobar/lung collapse, or nodules | ||
| Origin of Edema | Not fully explained by cardiac failure or fluid overload | ||
| Oxygenation (PaO₂/FiO₂) | 200-300 mmHg with PEEP ≥5 cm H₂O |
100-200 mmHg with PEEP ≥5 cm H₂O |
≤100 mmHg with PEEP ≥5 cm H₂O |
| Mortality Rate | 27% | 32% | 45% |
Additional Diagnostic Studies
- Arterial Blood Gas: Severe hypoxemia, respiratory alkalosis initially
- Chest X-ray: Bilateral patchy infiltrates
- Echocardiogram: Rule out cardiogenic cause
- Laboratory: Elevated LDH, decreased albumin
- CT Chest: Ground glass opacities, consolidation
Differential Diagnosis
- Cardiogenic pulmonary edema
- Pneumonia
- Pulmonary embolism
- Interstitial lung disease
- Acute interstitial pneumonia
- Drug-induced lung injury
Stages of ARDS Progression
Exudative Phase (Days 1-7)
Pathophysiology
- • Acute inflammatory response
- • Increased capillary permeability
- • Alveolar flooding with protein-rich fluid
- • Neutrophil activation and migration
Clinical Features
- • Rapid onset dyspnea
- • Severe hypoxemia
- • Bilateral infiltrates on CXR
- • Decreased lung compliance
Proliferative Phase (Days 7-21)
Pathophysiology
- • Fibroblast proliferation
- • Type II pneumocyte hyperplasia
- • Early collagen deposition
- • Organizing pneumonia pattern
Clinical Features
- • Persistent hypoxemia
- • Increased dead space ventilation
- • Progressive respiratory failure
- • Difficult weaning from ventilator
Fibrotic Phase (>21 Days)
Pathophysiology
- • Extensive pulmonary fibrosis
- • Alveolar architectural destruction
- • Pulmonary hypertension development
- • Permanent lung function impairment
Clinical Features
- • Persistent respiratory failure
- • High ventilatory requirements
- • Multiple organ dysfunction
- • Poor long-term prognosis
Clinical Significance
Understanding the phases of ARDS is crucial for nursing care planning. Early intervention during the exudative phase may prevent progression to fibrotic changes. Each phase requires different therapeutic approaches and has distinct prognostic implications for patient outcomes.
Comprehensive Nursing Assessment
Assessment Mnemonic: “BREATHE”
Breathing pattern
Respiratory rate
Examination findings
Arterial blood gas
Thinking/cognition
Hemodynamics
Electrolytes/labs
Primary Assessment Priorities
Airway & Breathing
- • Respiratory rate, rhythm, depth
- • Use of accessory muscles
- • Breath sounds (bilateral assessment)
- • Oxygen saturation (SpO₂)
- • Arterial blood gas analysis
Circulation
- • Heart rate and rhythm
- • Blood pressure (arterial line preferred)
- • Central venous pressure
- • Capillary refill time
- • Peripheral pulses and edema
Secondary Assessment Components
Neurological Status
- • Level of consciousness (GCS)
- • Orientation and cognition
- • Anxiety and agitation levels
- • Pupil response and reflexes
Skin & Comfort
- • Skin color and temperature
- • Diaphoresis and cyanosis
- • Pain assessment (0-10 scale)
- • Pressure injury risk
Monitoring Parameters for ARDS
| Parameter | Normal Range | ARDS Findings | Frequency |
|---|---|---|---|
| SpO₂ | 95-100% | <88% despite high FiO₂ | Continuous |
| PaO₂/FiO₂ Ratio | 400-500 mmHg | <300 mmHg | q4-6h or PRN |
| Respiratory Rate | 12-20/min | >30/min | Continuous |
| PEEP | 5 cm H₂O | 10-20 cm H₂O | Per protocol |
| Plateau Pressure | <30 cm H₂O | Often >30 cm H₂O | With each ABG |
Evidence-Based Nursing Interventions
Intervention Priority: “SUPPORT”
Sedation management
Unload the heart
Prevent complications
Positioning therapy
Ooxygenation optimize
Restrict fluids
Trend monitoring
Respiratory Management
Oxygen Therapy
- • Maintain SpO₂ 88-95% (avoid hyperoxemia)
- • Use lowest FiO₂ to achieve target
- • Consider high-flow nasal cannula if appropriate
- • Monitor for oxygen toxicity signs
Positioning Strategies
- • Prone positioning 12-16 hours daily
- • Semi-Fowler’s position when supine
- • Frequent position changes q2h
- • Avoid prolonged supine positioning
Fluid and Hemodynamic Management
Conservative Fluid Strategy
- • Target CVP 4-6 mmHg or PAWP 8-12 mmHg
- • Daily fluid balance assessment
- • Consider diuretics per protocol
- • Monitor electrolyte levels closely
Hemodynamic Monitoring
- • Continuous cardiac monitoring
- • Arterial line for frequent ABGs
- • Central venous access as needed
- • Pulmonary artery catheter if indicated
Sedation and Comfort Management
Sedation Protocols
- • Light sedation preferred (RASS -1 to 0)
- • Daily sedation interruption trials
- • Avoid excessive sedation
- • Consider dexmedetomidine for ICU delirium
Pain and Anxiety
- • Regular pain assessment using valid scales
- • Multimodal analgesia approach
- • Non-pharmacological comfort measures
- • Family presence and communication
Complication Prevention
Infection Prevention
- • Strict hand hygiene
- • VAP prevention bundle
- • Sterile technique procedures
- • Daily assessment for extubation
Skin Integrity
- • Pressure injury prevention
- • Skin assessment q4h
- • Proper positioning aids
- • Moisture management
DVT Prevention
- • Sequential compression devices
- • Early mobilization when stable
- • Pharmacological prophylaxis
- • Regular assessment for signs
Critical Nursing Considerations
Patients with ARDS require intensive monitoring and rapid response to changes. Early recognition of deterioration and prompt intervention can significantly impact outcomes. Always maintain open communication with the healthcare team and be prepared for emergency situations including sudden desaturation or hemodynamic instability.
Mechanical Ventilation in ARDS
Lung-Protective Ventilation Strategy
The cornerstone of ARDS management involves lung-protective mechanical ventilation to minimize ventilator-induced lung injury while maintaining adequate gas exchange.
Low Tidal Volume Strategy
Target Parameters
- • Tidal Volume: 6 mL/kg predicted body weight
- • Plateau Pressure: ≤30 cm H₂O
- • Driving Pressure: <15 cm H₂O (Pplat - PEEP)
- • pH: 7.30-7.45 (permissive hypercapnia)
Predicted Body Weight Formula
Male: 50 + 2.3 × (height in inches – 60)
Female: 45.5 + 2.3 × (height in inches – 60)
PEEP Management
PEEP Titration Goals
- • Maintain alveolar recruitment
- • Minimize FiO₂ requirements
- • Avoid overdistension
- • Monitor hemodynamic effects
| FiO₂ | PEEP (cm H₂O) |
|---|---|
| 0.3 | 5 |
| 0.4 | 8 |
| 0.5 | 10 |
| 0.6 | 12 |
| 0.7 | 14 |
| 0.8 | 16 |
| 0.9 | 18 |
| 1.0 | 20-24 |
Preferred Ventilator Modes
Volume Control (VC)
- • Guaranteed tidal volume delivery
- • Allows pressure monitoring
- • Preferred for lung protection
- • Risk of high airway pressures
Pressure Control (PC)
- • Limits peak airway pressure
- • Variable tidal volume
- • Better pressure distribution
- • Requires close monitoring
Pressure Support (PS)
- • Patient-triggered breaths
- • Reduces work of breathing
- • Weaning mode
- • Requires spontaneous effort
Advanced Ventilation Strategies
Recruitment Maneuvers
- • Applied PEEP 35-40 cm H₂O for 30-40 seconds
- • Used to recruit collapsed alveoli
- • Monitor hemodynamic response
- • Consider in severe hypoxemia
High-Frequency Oscillation
- • Very small tidal volumes (1-4 mL/kg)
- • High respiratory rates (300-900/min)
- • Reserved for refractory cases
- • Specialized equipment required
Inverse Ratio Ventilation
- • Inspiratory time > expiratory time
- • Improves oxygenation
- • May cause auto-PEEP
- • Requires heavy sedation
Extracorporeal Support
- • ECMO for severe refractory cases
- • VV-ECMO for respiratory failure
- • Bridge to recovery or transplant
- • Specialized center management
Ventilator Assessment Mnemonic: “VENTS”
V – Volumes
- • Tidal volume
- • Minute ventilation
- • Dead space
E – Exchange
- • Gas exchange
- • V/Q matching
- • Shunt fraction
N – Numbers
- • Respiratory rate
- • I:E ratio
- • Flow settings
T – Triggers
- • Sensitivity
- • Patient effort
- • Synchrony
S – Safety
- • Alarm limits
- • Pressure limits
- • Backup ventilation
Complications of ARDS
Early Recognition is Critical
ARDS patients are at high risk for multiple complications that can significantly impact mortality and long-term outcomes. Vigilant nursing assessment and early intervention are essential for preventing and managing these complications.
Immediate Complications (Hours to Days)
Pneumothorax
Incidence: 10-15% of mechanically ventilated patients
Signs: Sudden desaturation, increased peak pressures, absent breath sounds
Nursing Actions: Immediate assessment, prepare for chest tube insertion
Hemodynamic Instability
Causes: High PEEP, decreased venous return, sepsis
Signs: Hypotension, decreased cardiac output, oliguria
Management: Fluid optimization, vasopressor support
Ventilator-Associated Pneumonia
Risk: 15-25% of mechanically ventilated patients
Prevention: VAP bundle implementation
Signs: New infiltrates, purulent secretions, fever
Long-term Complications (Weeks to Months)
ICU-Acquired Weakness
Incidence: 25-50% of critically ill patients
Risk Factors: Prolonged bed rest, corticosteroids, neuromuscular blocking agents
Prevention: Early mobility, physical therapy
Pulmonary Fibrosis
Development: Progressive fibrotic phase of ARDS
Impact: Reduced lung compliance, prolonged ventilation
Monitoring: Serial imaging, pulmonary function tests
Post-ICU Syndrome
Components: Cognitive, physical, and psychological impairments
Duration: Can persist for months to years
Support: Multidisciplinary rehabilitation approach
Evidence-Based Prevention Strategies
| Complication | Prevention Bundle | Nursing Interventions | Monitoring |
|---|---|---|---|
| VAP |
• Head of bed elevation • Daily sedation breaks • Oral care protocol • Subglottic secretion drainage |
• Q4h oral care • Sedation assessment • Extubation readiness • Hand hygiene |
• Sputum characteristics • Chest X-ray changes • Temperature trends • WBC count |
| DVT/PE |
• Pharmacological prophylaxis • Mechanical prophylaxis • Early mobilization • Risk assessment |
• Sequential compression devices • Range of motion exercises • Leg assessment • Mobility progression |
• Calf swelling/pain • Sudden dyspnea • D-dimer levels • Doppler studies |
| Pressure Injuries |
• Risk assessment tools • Pressure redistribution • Skin inspection • Nutrition optimization |
• Q2h repositioning • Skin care protocol • Pressure-relieving surfaces • Moisture management |
• Daily skin assessment • Braden scale scoring • Nutrition status • Equipment pressure points |
Prognosis and Recovery
Survival Rates
Overall mortality has improved significantly over the past decades:
- • 1990s: 50-60% mortality
- • 2000s: 40-50% mortality
- • Current: 35-46% mortality
- • Mild ARDS: 27% mortality
- • Severe ARDS: 45% mortality
Prognostic Factors
Better Prognosis
- • Younger age (<50 years)
- • Direct lung injury
- • Higher PaO₂/FiO₂ ratio
- • Lower APACHE II score
- • Early recognition
Worse Prognosis
- • Advanced age (>65 years)
- • Sepsis-induced ARDS
- • Multiple organ failure
- • Immunocompromised status
- • Delayed treatment
Recovery Timeline
Acute Phase (1-2 weeks)
Intensive care management, mechanical ventilation, organ support. Focus on survival and preventing complications.
Stabilization Phase (2-8 weeks)
Weaning from mechanical ventilation, early mobilization, rehabilitation begins. Recovery of basic functions.
Recovery Phase (3-12 months)
Gradual improvement in lung function, physical rehabilitation, return to activities of daily living.
Long-term Phase (1+ years)
Continued improvement possible, some patients may have persistent limitations. Long-term follow-up essential.
Long-term Health Outcomes
Pulmonary Function
- • 70% have normal lung function at 1 year
- • Decreased exercise tolerance common
- • Some develop chronic restrictive disease
- • Improved outcomes with early mobilization
Physical Function
- • Muscle weakness and fatigue
- • Joint stiffness and pain
- • Decreased functional capacity
- • Benefits from structured rehabilitation
Quality of Life
- • Depression and anxiety common
- • PTSD in 25% of survivors
- • Cognitive impairment possible
- • Family support crucial
Rehabilitation Priorities
Physical Rehabilitation
- • Progressive mobility program
- • Respiratory muscle training
- • Strength and endurance building
- • Balance and coordination exercises
- • Occupational therapy for ADLs
Psychological Support
- • Mental health screening
- • Counseling and therapy
- • Support groups
- • Family counseling
- • Stress management techniques
Nursing Role in Recovery
Nurses play a pivotal role throughout the ARDS recovery continuum. From acute care management to discharge planning and follow-up coordination, nursing interventions significantly impact patient outcomes. Early mobility, family support, medication management, and patient education are key components of comprehensive nursing care that promote optimal recovery.
Global Best Practices in ARDS Management
International Collaboration in ARDS Care
Healthcare systems worldwide have developed innovative approaches to ARDS management, sharing evidence-based practices that have improved patient outcomes globally.
European Intensive Care Society (ESICM) Guidelines
Early Mobilization Protocol
- • Standardized assessment tools (ICU-CAM, RASS)
- • Multidisciplinary team approach
- • Progressive mobility algorithm
- • Outcomes tracking and quality improvement
- • Result: 30% reduction in ICU length of stay
Prone Positioning Excellence
- • Specialized prone positioning teams
- • Extended prone sessions (16-20 hours)
- • Safety protocols and equipment standards
- • Nursing competency certification programs
- • Impact: 20% mortality reduction in severe ARDS
Australia & New Zealand ICU (ANZICS) Innovation
ECMO Network Excellence
- • Centralized ECMO coordination system
- • 24/7 retrieval and transport services
- • Standardized patient selection criteria
- • Continuous quality monitoring
- • Achievement: Highest ECMO survival rates globally
Family-Centered Care Model
- • Unrestricted family visiting policies
- • Family participation in care decisions
- • Dedicated family support coordinators
- • Structured communication protocols
- • Outcome: Improved patient and family satisfaction
Asian Critical Care Innovation
Japan’s Technology Integration
- • AI-assisted ventilator weaning protocols
- • Real-time lung imaging technology
- • Automated PEEP optimization systems
- • Electronic health record integration
- • Innovation: 25% faster weaning times
Singapore’s Nurse-Led Protocols
- • Advanced practice nurse specialists
- • Nurse-driven sedation protocols
- • Independent nursing assessments
- • Continuous professional development
- • Result: Improved patient outcomes and satisfaction
North American Excellence Centers
Mayo Clinic ARDS Protocol
- • Predictive analytics for early identification
- • Personalized medicine approaches
- • Biomarker-guided therapy
- • Comprehensive survivorship programs
- • Innovation: 40% reduction in time to diagnosis
Johns Hopkins ARDS Recovery
- • Post-ICU syndrome prevention programs
- • Integrated rehabilitation services
- • Telemedicine follow-up systems
- • Research-practice integration
- • Impact: 50% improvement in quality of life scores
Emerging Global Trends
Artificial Intelligence
- • Predictive modeling for ARDS risk
- • Machine learning for ventilator settings
- • Pattern recognition in chest imaging
- • Clinical decision support systems
Precision Medicine
- • Genomic profiling for treatment selection
- • Biomarker-guided therapy
- • Personalized ventilation strategies
- • Targeted pharmacological interventions
Telemedicine Integration
- • Remote ICU monitoring systems
- • Specialist consultation networks
- • Virtual family conferences
- • Post-discharge follow-up programs
Key Success Factors Across Global Programs
Team Collaboration
Multidisciplinary approach with clear communication
Evidence-Based Protocols
Standardized, research-supported practices
Continuous Improvement
Quality monitoring and outcome tracking
Education Focus
Ongoing training and competency development
Implementing Global Best Practices
Healthcare institutions worldwide continue to share innovations in ARDS management through international collaborations, research networks, and professional organizations. Nurses play a crucial role in implementing these evidence-based practices at the bedside, adapting global standards to local contexts while maintaining quality and safety standards. The future of ARDS care lies in continued international cooperation and knowledge sharing.