
Care Coordination in Hospital Medication Reconciliation and Administration
A Comprehensive Nursing Study Guide
Introduction to Medication Reconciliation
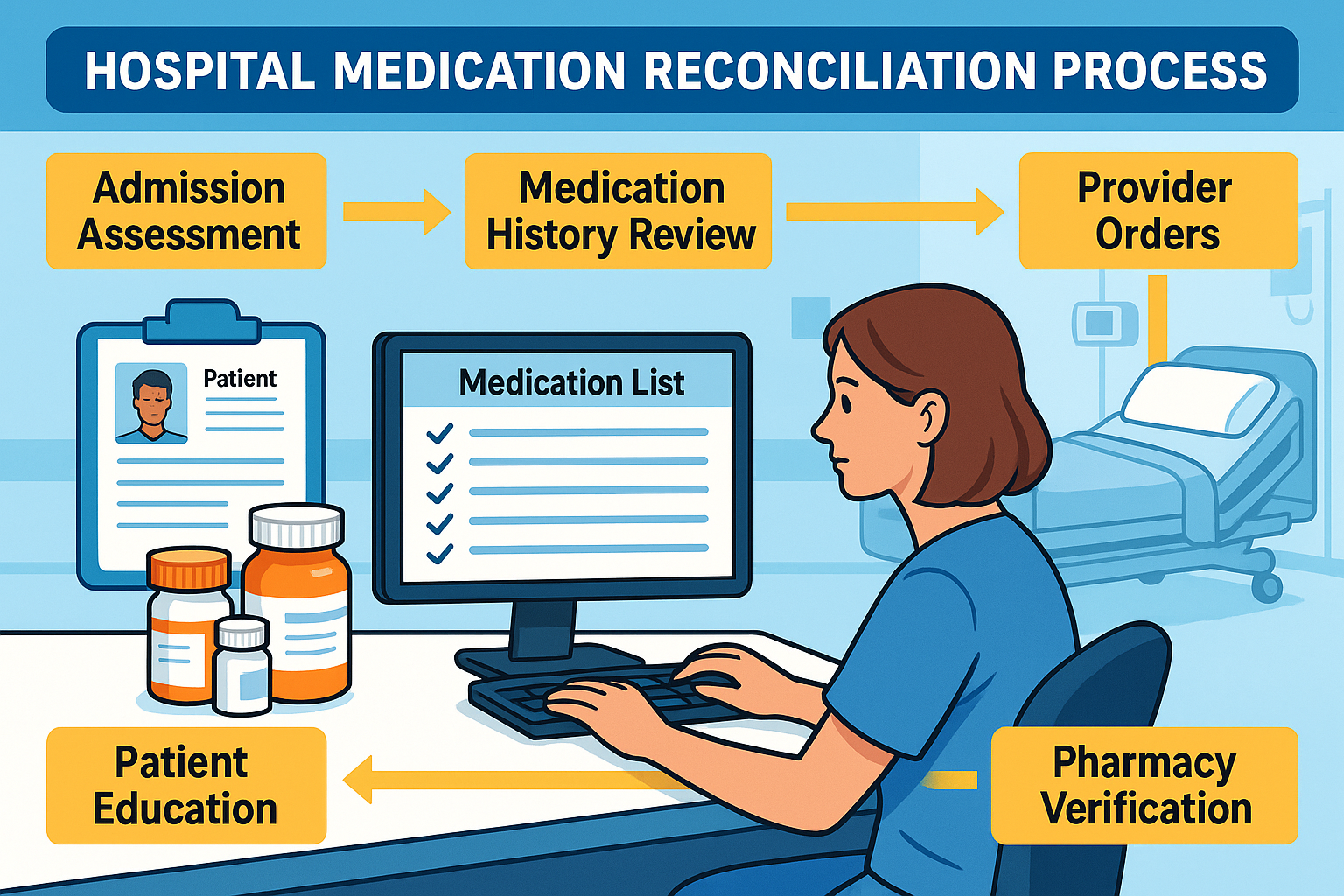
Medication reconciliation represents one of the most critical safety processes in hospital care coordination. This systematic approach ensures accurate and complete medication information transfer across care transitions, directly impacting patient outcomes and reducing adverse drug events. As a nursing professional, understanding the intricacies of medication reconciliation within the broader framework of care coordination is essential for delivering safe, effective patient care.
Definition Deep Dive
Medication reconciliation is the process of creating the most accurate list possible of all medications a patient is taking and comparing that list against the physician’s admission, transfer, and/or discharge orders, with the goal of providing correct medications to the patient at all transition points within the hospital.
The Foundation of Safe Care
Hospital-based medication reconciliation serves as the cornerstone of medication safety, with studies indicating that up to 67% of medication histories contain at least one error. These discrepancies can lead to medication errors, adverse drug events, and compromised patient safety. The medication reconciliation process involves three critical steps: verification, clarification, and reconciliation of medication orders across care transitions.
Care coordination in this context extends beyond simple documentation—it requires seamless communication between healthcare team members, patients, families, and external healthcare providers. The nursing role encompasses assessment, advocacy, education, and continuous monitoring throughout the patient’s hospital journey.
Memory Aid: RECONCILE
- Review all current medications
- Evaluate for accuracy and completeness
- Communicate with patient and family
- Obtain medication history from multiple sources
- Notify providers of discrepancies
- Clarify unclear orders
- Intentional decision-making for each medication
- List must be current and accurate
- Educate patient on changes
Care Coordination Framework
Effective care coordination for medication reconciliation requires a structured, interprofessional approach that integrates nursing expertise with collaborative team dynamics. This framework ensures comprehensive medication management while promoting patient safety and optimal outcomes.
Interprofessional Team Roles
Nursing Responsibilities
- • Conduct comprehensive medication history interviews
- • Verify medication information with multiple sources
- • Assess patient understanding of medications
- • Monitor for adverse drug reactions
- • Educate patients on medication changes
- • Document medication reconciliation activities
Physician Responsibilities
- • Review and approve medication lists
- • Make intentional prescribing decisions
- • Address medication discrepancies
- • Provide clinical rationale for changes
- • Collaborate on complex cases
- • Ensure appropriate monitoring parameters
Pharmacist Responsibilities
- • Clinical medication review and analysis
- • Drug interaction screening
- • Dosing recommendations
- • Therapeutic duplicate identification
- • Medication counseling support
- • Formulary guidance
Patient and Family Roles
- • Provide accurate medication history
- • Bring current medication bottles
- • Share over-the-counter medications
- • Report allergies and adverse reactions
- • Ask questions about changes
- • Participate in medication education
Communication Strategies
| Communication Method | Best Practices | Key Benefits |
|---|---|---|
| Bedside Rounds | Include patient in discussions, use teach-back method | Real-time clarification, patient engagement |
| SBAR Reports | Structured communication format for medication changes | Clear, concise information transfer |
| Electronic Alerts | Configure meaningful alerts, avoid alert fatigue | Automated safety checks, timely notifications |
| Phone Consultations | Document all verbal orders, read-back verification | Immediate response to urgent issues |
Pro Tip: The Golden Hour
Complete initial medication reconciliation within the first hour of admission. This “golden hour” approach significantly reduces medication errors and establishes a foundation for safe care throughout the hospitalization.
Admission Medication Reconciliation
The admission phase represents the most critical opportunity for comprehensive medication reconciliation. This process sets the foundation for safe medication management throughout the patient’s hospital stay and requires meticulous attention to detail and systematic approach.
Systematic Admission Process
Step 1: Data Collection
Gather comprehensive medication history from multiple sources
Step 2: Verification
Cross-reference information and identify discrepancies
Step 3: Documentation
Record accurate, complete medication list in EHR
Information Sources Hierarchy
Patient/Family Interview
Direct conversation with patient or reliable family member
Medication Bottles/Lists
Physical medications brought by patient
Electronic Health Records
Previous hospitalizations and clinic visits
Pharmacy Records
Community pharmacy dispensing history
Primary Care Provider
Consultation with outpatient providers
Common Admission Challenges
High-Risk Scenarios
- • Emergency department admissions
- • Patients with cognitive impairment
- • Multiple pharmacy sources
- • Recent medication changes
- • Complex medication regimens
- • Language barriers
Solution Strategies
- • Use professional interpreters
- • Contact multiple family members
- • Verify with pharmacy networks
- • Review insurance claims data
- • Consult specialists when needed
- • Document uncertainty clearly
Memory Aid: ADMIT Protocol
- Assess patient and gather history
- Document all current medications
- Match with provider orders
- Identify discrepancies
- Take action to resolve differences
Transfer and Transition Processes
Patient transfers within the hospital present unique challenges for medication reconciliation and care coordination. Each transition point increases the risk of medication errors, making systematic processes essential for maintaining continuity and safety.
Types of Hospital Transfers
Unit to Unit
Medical-surgical to ICU
ICU Transfers
Critical care transitions
Surgical Units
Pre/post-operative care
Facility Transfer
Hospital to hospital
Transfer Medication Reconciliation Workflow
Pre-Transfer Assessment
Review current medication orders, recent changes, and ongoing treatments. Assess for time-sensitive medications and continuous infusions.
Communication Handoff
Provide structured report to receiving unit including medication changes, allergies, and special considerations using standardized format.
Receiving Unit Verification
Verify all medications against sending unit documentation, confirm continuation of critical medications, and assess for unit-specific protocols.
Documentation Update
Update electronic health record with transfer notes, medication reconciliation completion, and any identified discrepancies or concerns.
Critical Transfer Considerations
| Transfer Type | Key Focus Areas | Special Considerations |
|---|---|---|
| ICU to Med-Surg | Vasopressor weaning, sedation changes | Monitoring parameter adjustments |
| Med-Surg to ICU | Medication intensification, IV conversions | Critical care protocols |
| Post-Surgical | Pain management, anticoagulation | Surgical complications |
| Emergency Transfer | Time-critical medications | Rapid response protocols |
Best Practice: PASS the BATON
Patient summary
Action list
Situation assessment
Safety concerns
Background information
Actions taken
Timing considerations
Ownership/responsibility
Next actions needed
Medication Administration Coordination
Medication administration represents the final step in the medication reconciliation process, where coordinated care translates into direct patient intervention. This phase requires precise timing, accurate dosing, and continuous monitoring to ensure therapeutic effectiveness and patient safety.
Five Rights Plus Framework
Right Patient
Two identifiers verification
Right Drug
Correct medication selection
Right Dose
Accurate calculation
Right Route
Appropriate pathway
Right Time
Scheduled timing
Right Documentation
Complete recording
Right Reason
Clinical indication
Right Response
Monitor outcomes
Administration Scheduling Coordination
| Time Category | Medication Examples | Coordination Points |
|---|---|---|
| Time-Critical | Antibiotics, cardiac medications | ±30 minutes maximum variance |
| Non-Time-Critical | Vitamins, routine medications | ±2 hours acceptable variance |
| PRN Medications | Pain relievers, anti-nausea | Assessment-based timing |
| STAT Orders | Emergency medications | Immediate administration |
Technology Integration
Barcode Medication Administration
- • Patient wristband scanning
- • Medication package verification
- • Automated documentation
- • Real-time allergy alerts
- • Dosing verification
Smart Pump Technology
- • Dose error reduction systems
- • Drug library integration
- • Infusion monitoring
- • Wireless data transmission
- • Alarm management
Memory Aid: BEFORE Administration
- Barcode scan patient and medication
- Evaluate patient condition and vital signs
- Five rights verification complete
- Order verification and allergy check
- Reason for medication understood
- Educate patient about medication
High-Alert Medications
These medications require special handling procedures and double-verification protocols:
Anticoagulants: Heparin, warfarin
Insulin: All formulations
Opioids: IV morphine, fentanyl
Chemotherapy: All agents
Electrolytes: Concentrated KCl, MgSO4
Vasoactive drugs: Dopamine, epinephrine
Neuromuscular blockers
Hypoglycemic agents
IV moderate sedation agents
Discharge Medication Reconciliation
Discharge medication reconciliation represents the critical transition from hospital to community care. This process ensures patients receive accurate medication instructions, understand their therapy, and maintain continuity with their outpatient providers. Effective discharge coordination significantly reduces readmission rates and improves patient outcomes.
Comprehensive Discharge Process
Reconciliation
Compare admission to discharge medications
Education
Teach patients about changes and new medications
Communication
Contact primary care and pharmacy
Follow-up
Schedule post-discharge appointments
Medication Categories at Discharge
| Category | Action Required | Patient Education Focus |
|---|---|---|
| Continue Same | Resume pre-admission medications | Confirm understanding of ongoing therapy |
| Modified Dose | Adjust existing medication strength | Emphasize dosing changes and rationale |
| New Medications | Add therapy for acute conditions | Complete medication education |
| Discontinued | Stop specific medications | Explain reasons for discontinuation |
| Temporary Hold | Suspend medication with restart criteria | Clarify duration and restart conditions |
Patient Education Framework
Teach-Back Method
- 1. Explain medication information clearly
- 2. Ask patient to repeat back in their own words
- 3. Clarify any misunderstandings
- 4. Repeat until patient demonstrates understanding
- 5. Document education provided
Show-and-Tell Technique
- 1. Show actual medication containers
- 2. Demonstrate proper administration
- 3. Have patient practice technique
- 4. Provide written instructions
- 5. Ensure access to supplies
Best Practice: Medication Reconciliation Brown Bag Review
Encourage patients to bring all their medications (prescription, over-the-counter, supplements) in a bag to their first post-discharge appointment for comprehensive review with their primary care provider.
Studies show this simple intervention reduces medication discrepancies by up to 40% and improves patient safety outcomes.
Post-Discharge Follow-up Coordination
24-48 Hours
- • Pharmacy follow-up call
- • Medication acquisition verification
- • Initial adherence assessment
- • Address immediate concerns
3-7 Days
- • Nursing follow-up call
- • Symptom monitoring
- • Side effect assessment
- • Care plan adjustments
1-2 Weeks
- • Primary care appointment
- • Medication reconciliation review
- • Laboratory monitoring
- • Long-term planning
Memory Aid: DISCHARGE MEDS
- Determine current medication needs
- Identify changes from admission
- Simplify regimen when possible
- Communicate with outpatient providers
- Handle insurance and cost issues
- Arrange pharmacy transfer
- Review with patient thoroughly
- Give written instructions
- Ensure understanding via teach-back
- Make follow-up appointments
- Explain when to call for help
- Document all education provided
- Schedule post-discharge medication review
Safety Measures and Error Prevention
Patient safety in medication reconciliation and administration requires multi-layered approaches, systematic error prevention strategies, and continuous quality improvement. Implementing comprehensive safety measures protects patients from preventable adverse drug events and supports positive healthcare outcomes.
Common Medication Errors
Omission Errors
- • Failure to continue home medications
- • Missed doses during transitions
- • Incomplete medication histories
Commission Errors
- • Duplicate therapy orders
- • Inappropriate medication additions
- • Wrong medication selection
Dosing Errors
- • Incorrect dose calculations
- • Unit conversion mistakes
- • Frequency errors
Route Errors
- • Wrong administration pathway
- • IV versus PO confusion
- • Topical application errors
Timing Errors
- • Delayed administration
- • Premature medication giving
- • Scheduling conflicts
Communication Errors
- • Incomplete handoff information
- • Unclear verbal orders
- • Documentation gaps
Swiss Cheese Model Application
Multiple Layers of Protection
Each safety layer has potential gaps, but multiple layers prevent errors from reaching patients
Prescriber
Order verification
Pharmacist
Clinical review
Nurse
Administration verification
Technology
System safeguards
Error Prevention Strategies
System-Based Interventions
- • Computerized provider order entry (CPOE)
- • Clinical decision support systems
- • Automated dispensing cabinets
- • Barcode medication administration
- • Smart IV pumps with dose limits
- • Electronic medication reconciliation
- • Real-time allergy checking
- • Duplicate therapy alerts
Human Factor Improvements
- • Standardized medication reconciliation forms
- • Independent double-checks for high-risk medications
- • Tall man lettering for look-alike drugs
- • Unit dose packaging systems
- • Structured communication protocols
- • Regular competency assessments
- • Fatigue management strategies
- • Interruption-free medication zones
Education and Training
- • Ongoing medication safety education
- • Simulation-based training programs
- • Error reporting and learning culture
- • Peer review processes
- • Patient safety rounds participation
- • Root cause analysis involvement
- • Best practice sharing sessions
- • Continuing education requirements
Never Events in Medication Management
These serious, preventable events should never occur in healthcare:
- • Wrong patient medication administration
- • Significant medication overdose
- • IV administration of oral medications
- • Administration of contraindicated medications
- • Failure to follow up critical test results
- • Medication reconciliation omissions
Technology and Documentation
Modern healthcare technology plays a pivotal role in supporting medication reconciliation and care coordination. Electronic health records, clinical decision support systems, and mobile health applications enhance accuracy, efficiency, and communication throughout the medication reconciliation process.
Electronic Health Record Integration
Core EHR Features
- • Comprehensive medication history access
- • Real-time allergy and interaction alerts
- • Automated medication reconciliation workflows
- • Provider communication tools
- • Patient portal integration
- • Quality measure tracking
Mobile Technology Benefits
- • Point-of-care medication verification
- • Barcode scanning capabilities
- • Voice recognition documentation
- • Instant messaging between providers
- • Photo documentation of medications
- • Secure communication platforms
Clinical Decision Support Systems
| Alert Type | Trigger Conditions | Nursing Actions |
|---|---|---|
| Drug Allergy | Known allergy to prescribed medication | Hold medication, contact prescriber immediately |
| Drug Interaction | Clinically significant medication interactions | Assess severity, consult pharmacist if needed |
| Dose Range | Dose exceeds recommended parameters | Verify order, confirm with prescriber |
| Duplicate Therapy | Multiple medications same therapeutic class | Review necessity, clarify intentional duplication |
| Renal Function | Nephrotoxic drug with kidney impairment | Monitor labs, assess dose appropriateness |
Documentation Best Practices
Accuracy Requirements
- • Complete medication names (avoid abbreviations)
- • Precise dosing including units
- • Specific administration routes
- • Exact timing parameters
- • Duration of therapy
Timeliness Standards
- • Real-time documentation preferred
- • Maximum 2-hour delay acceptable
- • Immediate entry for STAT medications
- • End-of-shift completion required
- • Prompt error reporting
Legal Considerations
- • Permanent electronic record
- • Cannot alter completed entries
- • Addendum for corrections
- • Authentication requirements
- • Privacy protection compliance
Technology Tip: Smart Alerts Management
Customize alert settings to reduce “alert fatigue” while maintaining safety. Work with IT departments to adjust sensitivity levels based on clinical relevance and unit-specific needs.
Hospitals using optimized alert systems report 23% fewer override rates and 31% better medication safety outcomes.
Emerging Technologies
Artificial Intelligence
- • Predictive medication reconciliation errors
- • Natural language processing for medication extraction
- • Machine learning for dosing optimization
- • Automated medication history compilation
Cloud-Based Solutions
- • Interoperable health information exchange
- • Real-time medication data sharing
- • Scalable care coordination platforms
- • Remote monitoring capabilities
Global Best Practices
Healthcare systems worldwide have developed innovative approaches to medication reconciliation and care coordination. Learning from international best practices enhances our understanding of effective strategies and provides insights for continuous improvement in patient safety and care quality.
International Success Models
United States: High Reliability Organizations
Key Strategies:
- • Just culture approach to error reporting
- • Systematic medication reconciliation processes
- • Advanced clinical decision support
- • Interprofessional care teams
Outcomes:
- • 40% reduction in medication errors
- • Improved patient satisfaction scores
- • Enhanced provider communication
- • Decreased readmission rates
Canada: Safer Healthcare Now! Initiative
Innovation Focus:
- • Standardized medication reconciliation toolkit
- • Best Possible Medication History (BPMH)
- • Provincial medication information systems
- • Community pharmacy partnerships
Results:
- • 95% BPMH completion rates
- • 50% reduction in unintended discrepancies
- • Enhanced care transitions
- • Improved medication adherence
United Kingdom: NHS Improvement Programme
System Approach:
- • Electronic prescribing and administration
- • Integrated care pathways
- • National medication safety alerts
- • Patient involvement in medication safety
Achievements:
- • 30% decrease in medication incidents
- • Improved clinical outcomes
- • Enhanced patient engagement
- • Cost-effective care delivery
Netherlands: Integrated Medication Management
Collaborative Model:
- • Hospital-community pharmacy integration
- • Shared medication records
- • Clinical pharmacist involvement
- • Patient-centered care approaches
Impact:
- • Seamless care transitions
- • Reduced medication-related problems
- • Improved health outcomes
- • Enhanced provider satisfaction
Emerging Global Trends
Digitalization Trends
- • Artificial intelligence integration
- • Blockchain for medication tracking
- • Internet of Things (IoT) monitoring
- • Telemedicine medication consultations
- • Mobile health applications
Patient-Centered Innovations
- • Patient-reported medication experiences
- • Personalized medication adherence programs
- • Cultural competency in medication counseling
- • Health literacy-appropriate materials
- • Shared decision-making models
Universal Principles for Excellence
- ✓ Standardized processes and protocols
- ✓ Technology-enabled safety systems
- ✓ Interprofessional collaboration
- ✓ Continuous quality improvement
- ✓ Patient and family engagement
- ✓ Evidence-based practice integration
- ✓ Performance measurement and feedback
- ✓ Culture of safety and learning
Implementation Strategies
Assessment Phase
- • Current state analysis
- • Gap identification
- • Stakeholder engagement
- • Resource assessment
Implementation Phase
- • Pilot program development
- • Staff training and education
- • Technology deployment
- • Process standardization
Sustainability Phase
- • Performance monitoring
- • Continuous improvement
- • Scale and spread
- • Culture reinforcement
Conclusion and Key Takeaways
Medication reconciliation and care coordination represent fundamental components of safe, effective hospital nursing practice. As healthcare becomes increasingly complex, the nursing role in coordinating medication management across care transitions becomes ever more critical to patient safety and optimal outcomes.
Essential Competencies for Success
Assessment Skills
Comprehensive medication history gathering and discrepancy identification
Communication
Effective interprofessional collaboration and patient education
Critical Thinking
Clinical reasoning and medication safety decision-making
Technology Proficiency
Electronic health record navigation and clinical decision support
Safety Mindset
Error prevention strategies and patient advocacy
Patient-Centered Care
Culturally competent and individualized medication management
Final Memory Aid: EXCELLENCE in Medication Reconciliation
- Evaluate medications comprehensively
- X-ray vision for discrepancies
- Communicate effectively with teams
- Educate patients thoroughly
- Listen to patient concerns
- Leverage technology appropriately
- Ensure safety at all transitions
- Never assume – always verify
- Coordinate care across settings
- Engage in continuous learning
Future Directions
The future of medication reconciliation and care coordination continues to evolve with advancing technology, changing healthcare delivery models, and growing emphasis on patient engagement. Nursing professionals must stay current with emerging trends while maintaining focus on fundamental safety principles.
Emerging Opportunities:
- • Artificial intelligence-assisted reconciliation
- • Wearable technology integration
- • Precision medicine applications
- • Genomic-guided medication therapy
Continuing Challenges:
- • Healthcare system fragmentation
- • Information technology interoperability
- • Resource allocation and staffing
- • Health equity and access issues
Your Commitment to Excellence
As a nursing professional, your dedication to accurate medication reconciliation and effective care coordination directly impacts patient safety and healthcare quality. Every medication history you take, every discrepancy you identify, and every educational moment you provide contributes to better patient outcomes.
Continue to advocate for your patients, collaborate with your healthcare team, and maintain the highest standards of medication safety. Your expertise and commitment make a difference in every patient’s healing journey.
Continue Your Learning Journey
Stay updated with evidence-based practices, participate in continuing education opportunities, and contribute to the advancement of medication safety in your healthcare organization.