
Gastrointestinal Tumors
Comprehensive Nursing Study Notes
Osmosis-Style Medical Education • Evidence-Based Learning
Nursing Students
Advanced Pathophysiology
Anatomical Overview of GI Tumors
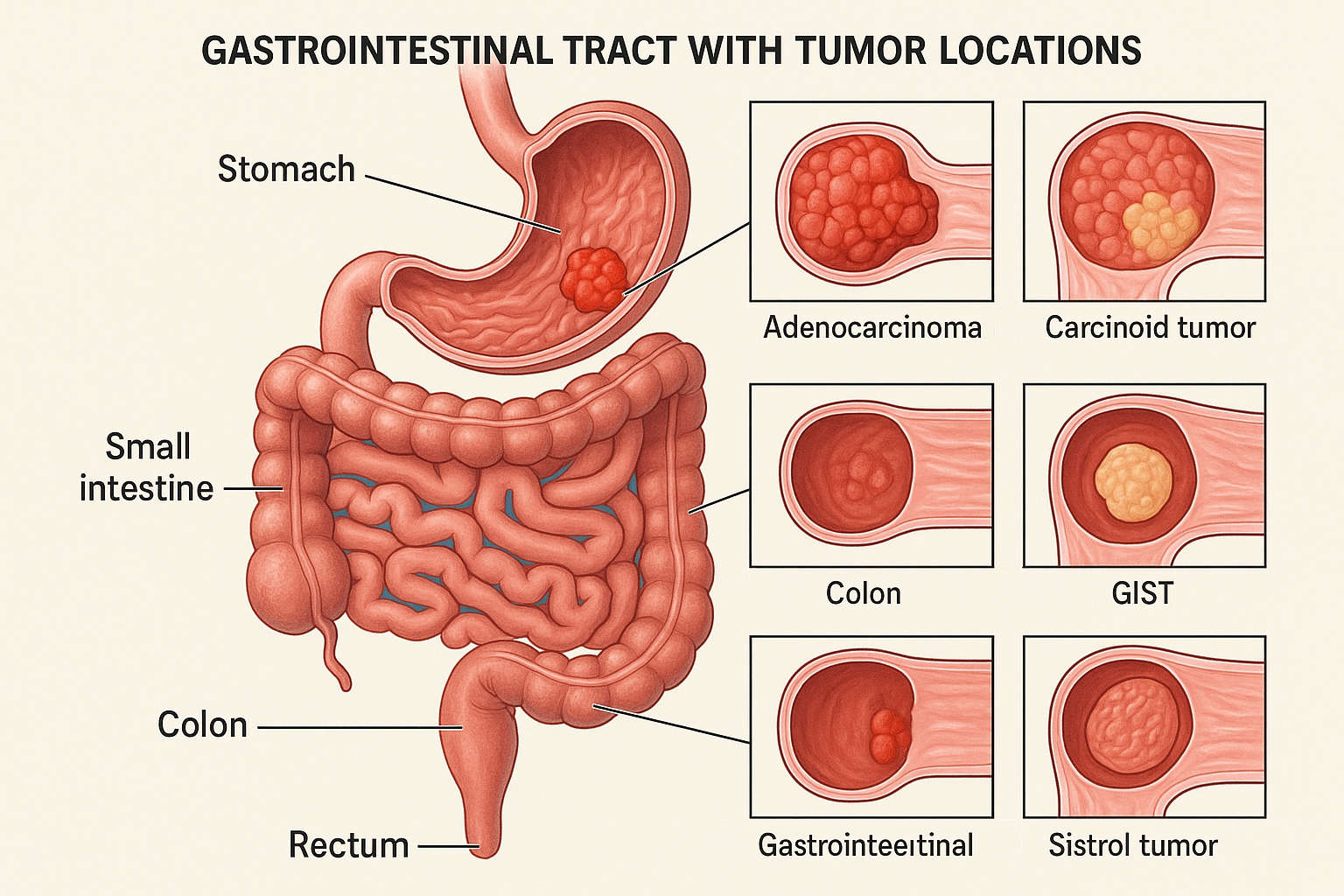
Comprehensive anatomical illustration showing common locations and types of gastrointestinal tumors
Table of Contents
1. Introduction & Overview
Gastrointestinal tumors represent a diverse group of neoplasms affecting the digestive tract from the esophagus to the anus. These tumors constitute a significant portion of cancer diagnoses worldwide, with colorectal cancer being the third most common cancer globally and gastric cancer ranking fourth in cancer-related mortality.
Key Statistical Facts
- Colorectal cancer: ~1.9 million new cases annually worldwide
- Gastric cancer: ~1.1 million new cases annually
- Pancreatic cancer: ~495,000 new cases annually
- Hepatocellular carcinoma: ~906,000 new cases annually
- 5-year survival rates vary dramatically by location and stage at diagnosis
Anatomical Regions Affected
Upper GI Tract
- • Esophagus
- • Stomach
- • Duodenum
- • Liver
- • Gallbladder
- • Pancreas
Lower GI Tract
- • Small intestine
- • Cecum
- • Colon
- • Rectum
- • Anal canal
Nursing Significance
Understanding GI tumors is crucial for nursing practice because nurses play pivotal roles in:
- Early recognition of symptoms and risk factors
- Pre- and post-operative care management
- Chemotherapy and radiation therapy support
- Nutritional assessment and intervention
- Pain management and comfort care
- Patient and family education
- Psychosocial support throughout the cancer journey
2. Classification of GI Tumors
Memory Aid: “CALM NETS”
Primary Classifications:
- Carcinomas (Adenocarcinoma, SCC)
- Adenocarcinoma (most common)
- Lymphomas (MALT, DLBCL)
- Melanoma (rare)
Specialized Types:
- Neuroendocrine tumors
- Epithelial tumors
- Tumors, stromal (GIST)
- Sarcomas (rare)
Detailed Classification by Histology
Adenocarcinomas (80-90% of GI cancers)
Arise from glandular epithelium; most common type in colon, rectum, stomach, and pancreas.
- Well-differentiated: Better prognosis, maintains glandular architecture
- Moderately differentiated: Intermediate prognosis
- Poorly differentiated: Aggressive behavior, poor prognosis
- Signet ring cell: Particularly aggressive subtype
Squamous Cell Carcinomas
More common in esophagus and anal canal; associated with smoking, alcohol, and HPV.
Neuroendocrine Tumors (NETs)
Previously called carcinoid tumors; can secrete hormones causing carcinoid syndrome.
- Grade 1 (G1): Well-differentiated, low proliferation rate
- Grade 2 (G2): Moderately differentiated
- Grade 3 (G3): Poorly differentiated, high proliferation
Gastrointestinal Stromal Tumors (GIST)
Arise from interstitial cells of Cajal; most common mesenchymal tumor of GI tract.
Lymphomas
Primary GI lymphomas account for 30-40% of extranodal lymphomas.
- MALT (Mucosa-Associated Lymphoid Tissue): Associated with H. pylori
- DLBCL (Diffuse Large B-Cell Lymphoma): More aggressive
- Mantle cell lymphoma: Can cause lymphomatous polyposis
3. Pathophysiology
Carcinogenesis Sequence: “MAIM”
Initial DNA damage
Oncogene activation
Tumor suppressor loss
Invasion & spread
Molecular Pathogenesis
Adenoma-Carcinoma Sequence (Colorectal Cancer)
Key Oncogenes and Tumor Suppressors
Oncogenes (Accelerator)
- KRAS: 40% of colorectal cancers, predicts anti-EGFR therapy resistance
- MYC: Promotes cell proliferation and angiogenesis
- HER2: 15-20% of gastric cancers, therapeutic target
- BRAF: 10% of colorectal cancers, poor prognosis
Tumor Suppressors (Brakes)
- APC: 80% of colorectal cancers, early event
- p53: 50-70% of GI cancers, “guardian of genome”
- SMAD4: 30% of pancreatic cancers
- CDKN2A: 90% of pancreatic cancers
Hallmarks of Cancer in GI Tumors
Growth Signals
- • Self-sufficiency
- • Growth factor independence
- • Oncogene activation
Cell Death Resistance
- • Apoptosis evasion
- • p53 dysfunction
- • DNA repair defects
Invasion & Metastasis
- • EMT activation
- • Matrix degradation
- • Angiogenesis
Clinical Correlation
Understanding these molecular pathways is crucial for nursing care because they determine treatment response, prognosis, and guide targeted therapies. For example, KRAS mutations predict resistance to anti-EGFR therapies like cetuximab, while HER2 overexpression in gastric cancer indicates potential benefit from trastuzumab therapy.
4. Clinical Presentation
Red Flag Symptoms: “ALARM BELLS”
- Anemia (unexplained iron deficiency)
- Loss of weight (unintentional >10%)
- Anorexia (loss of appetite)
- Recent onset of symptoms >45 years
- Masses (palpable abdominal)
- Bleeding (overt or occult)
- Emergency symptoms (obstruction)
- Lymphadenopathy
- Liver enlargement
- Swallowing difficulties (dysphagia)
Location-Specific Presentations
Esophageal Cancer
Early Symptoms
- • Progressive dysphagia
- • Initially to solids
- • Substernal discomfort
- • Food impaction sensation
Advanced Symptoms
- • Dysphagia to liquids
- • Significant weight loss
- • Regurgitation
- • Aspiration pneumonia
Late Signs
- • Hoarseness (RLN involvement)
- • Chest pain
- • Hematemesis
- • Supraclavicular nodes
Gastric Cancer
Early (Often Silent)
- • Vague epigastric pain
- • Early satiety
- • Mild dyspepsia
- • Often asymptomatic
Progressive Symptoms
- • Weight loss
- • Anorexia
- • Nausea/vomiting
- • Iron deficiency anemia
Advanced Disease
- • Palpable mass
- • Gastric outlet obstruction
- • Ascites
- • Virchow’s node
Pancreatic Cancer
Head Tumors
- • Painless jaundice (70%)
- • Pale stools
- • Dark urine
- • Courvoisier’s sign
Body/Tail Tumors
- • Epigastric pain
- • Back pain
- • Weight loss
- • New-onset diabetes
General Features
- • Trousseau’s syndrome
- • Depression
- • Steatorrhea
- • Migratory thrombosis
Colorectal Cancer
Right-Sided Colon
- • Iron deficiency anemia
- • Fatigue
- • Occult bleeding
- • Palpable mass
Left-Sided Colon
- • Change in bowel habits
- • Decreased stool caliber
- • Obstruction symptoms
- • Visible blood in stool
Rectal Cancer
- • Rectal bleeding
- • Tenesmus
- • Change in stool caliber
- • Pelvic pain
Nursing Assessment Priorities
Systematic Assessment
- • Comprehensive pain assessment (location, quality, timing)
- • Nutritional status and weight trends
- • Bowel movement patterns and characteristics
- • Functional status and performance level
Psychosocial Factors
- • Anxiety and depression screening
- • Family support systems
- • Coping mechanisms
- • Knowledge deficits and learning needs
5. Diagnostic Methods
Diagnostic Approach: “LABS FIRST”
- Lab tests (CBC, CMP, tumor markers)
- Anatomy imaging (CT, MRI)
- Biopsy (tissue diagnosis)
- Staging workup
- Functional imaging (PET scan)
- Intestinal evaluation (colonoscopy)
- Risk assessment (genetic testing)
- Specialized tests (molecular markers)
- Tumor board review
Laboratory Tests
Routine Laboratory Studies
- • Hemoglobin/Hematocrit (anemia)
- • White blood cell count (infection, chemotherapy effects)
- • Platelet count (bleeding risk, chemotherapy effects)
- • Liver function tests (metastases, obstruction)
- • Renal function (contrast studies, chemotherapy)
- • Electrolytes (malnutrition, treatment effects)
Tumor Markers
Imaging Studies
Imaging Algorithm for GI Tumors
Clinical symptoms + Physical exam
EGD + CT chest/abdomen
Colonoscopy + CT abdomen/pelvis
MRI/MRCP + ERCP if needed
PET-CT + specialized imaging
CT Scan
- • Primary tumor assessment
- • Lymph node evaluation
- • Metastases detection
- • Treatment planning
- • Response monitoring
MRI
- • Liver lesion characterization
- • Rectal cancer staging
- • Pancreatic ductal evaluation
- • Soft tissue contrast
- • No radiation exposure
PET-CT
- • Metabolic activity assessment
- • Distant metastases detection
- • Treatment response evaluation
- • Recurrence surveillance
- • Prognostic information
Endoscopic Procedures
Upper Endoscopy (EGD)
- • Dysphagia, odynophagia
- • Upper GI bleeding
- • Persistent dyspepsia >45 years
- • Suspicious imaging findings
- • Direct visualization
- • Biopsy sampling
- • Therapeutic interventions
- • Endoscopic ultrasound (EUS)
Colonoscopy
- • Average risk: Start age 50 (updated to 45)
- • High risk: Earlier and more frequent
- • Family history: 10 years before affected relative
- • IBD: 8-10 years after diagnosis
- • 95% sensitive for large polyps
- • 90% sensitive for cancer
- • Gold standard for CRC screening
- • Therapeutic (polypectomy)
Nursing Considerations for Diagnostic Procedures
Pre-procedure
- • NPO status verification
- • Bowel preparation compliance
- • Medication reconciliation (anticoagulants)
- • Consent and patient education
- • Anxiety assessment and management
Post-procedure
- • Vital sign monitoring
- • Sedation recovery assessment
- • Complication surveillance (bleeding, perforation)
- • Discharge education
- • Follow-up care coordination
6. Treatment Approaches
Multimodal Treatment: “SCRIPT”
- Surgery (curative intent)
- Chemotherapy (systemic)
- Radiation therapy
- Immunotherapy
- Palliative care
- Targeted therapy
Surgical Management
Surgical Decision Algorithm
Location, Stage, Resectability
Curative resection
Neoadjuvant therapy
Palliative procedures
Curative Procedures
- • Esophagectomy (Ivor Lewis, McKeown)
- • Minimally invasive approaches
- • Endoscopic resection (early tumors)
- • Subtotal gastrectomy
- • Total gastrectomy
- • D1/D2 lymphadenectomy
- • Hemicolectomy (right/left)
- • Low anterior resection
- • Abdominoperineal resection
Palliative Procedures
- • Stent placement
- • Bypass surgery
- • Colostomy/ileostomy
- • Endoscopic therapy
- • Angiographic embolization
- • Palliative resection
- • Gastrostomy tube
- • Jejunostomy tube
- • Biliary drainage
Systemic Therapy
Chemotherapy Regimens
Colorectal Cancer
Gastric Cancer
Pancreatic Cancer
Targeted Therapies
EGFR Inhibitors
VEGF Inhibitors
Immunotherapy
PD-1/PD-L1 Inhibitors
Biomarkers
Nursing Management During Treatment
Chemotherapy Care
- • Pre-medication protocols
- • Infusion monitoring
- • Extravasation prevention
- • Side effect management
- • Patient education
Surgical Care
- • Preoperative optimization
- • Enhanced recovery protocols
- • Postoperative monitoring
- • Complication prevention
- • Discharge planning
Supportive Care
- • Symptom management
- • Nutritional support
- • Psychosocial care
- • Family support
- • Care coordination
7. Nursing Care & Management
Holistic Nursing Care: “COMFORT”
- Communication (therapeutic, family)
- Optimal symptom management
- Monitoring for complications
- Functional status maintenance
- Organized care coordination
- Respect for patient autonomy
- Teaching and education
Assessment Priorities
Systematic Nursing Assessment
- • Pain assessment
- • Nutritional status
- • Functional capacity
- • Symptom burden
- • Anxiety/depression
- • Coping mechanisms
- • Quality of life
- • Body image concerns
- • Support systems
- • Financial concerns
- • Role changes
- • Communication needs
- • Meaning/purpose
- • Religious needs
- • Hope/despair
- • End-of-life concerns
Evidence-Based Nursing Interventions
Pain Management
- • Numeric rating scale (0-10)
- • FACES scale for cognitive impairment
- • Behavioral indicators
- • Comprehensive pain history
- • Multimodal analgesia
- • Non-pharmacological methods
- • Patient-controlled analgesia (PCA)
- • Breakthrough pain management
Nutritional Support
- • BMI and weight trends
- • Albumin and prealbumin levels
- • Dietary intake evaluation
- • Malnutrition screening tools
- • Early dietitian consultation
- • Oral nutritional supplements
- • Enteral/parenteral nutrition
- • Managing taste changes
Infection Prevention
- • Immunosuppression from chemotherapy
- • Neutropenia
- • Central venous catheters
- • Surgical wounds
- • Hand hygiene compliance
- • Neutropenia precautions
- • Catheter care protocols
- • Early infection recognition
Chemotherapy-Specific Nursing Care
Common Side Effects Management
- • Prophylactic antiemetics (ondansetron, dexamethasone)
- • Dietary modifications (small, frequent meals)
- • Environmental controls (reduce odors)
- • Complementary therapies (ginger, acupressure)
- • Loperamide for mild symptoms
- • BRAT diet modifications
- • Fluid and electrolyte monitoring
- • Perineal skin care
Peripheral Neuropathy
- • CTCAE grading scale
- • Functional impact evaluation
- • Safety risk assessment
- • Quality of life measures
- • Dose modifications
- • Neuropathic pain medications
- • Safety education (fall prevention)
- • Occupational therapy referral
Emergency Recognition and Response
Febrile Neutropenia
- • Temperature >100.4°F + ANC <1000
- • Immediate blood cultures
- • Empiric antibiotics within 1 hour
- • Isolation precautions
Bowel Obstruction
- • Abdominal distension
- • Nausea/vomiting
- • Absence of flatus
- • NPO, NG decompression
Tumor Lysis Syndrome
- • Hyperkalemia, hyperphosphatemia
- • Hypocalcemia, hyperuricemia
- • Aggressive hydration
- • Allopurinol prophylaxis
8. Complications
Major Complications: “PROBLEMS”
- Perforation
- Recurrence/Relapse
- Obstruction (bowel, biliary)
- Bleeding (acute, chronic)
- Lymphatic spread
- Emergency situations
- Metastases (liver, lung, peritoneum)
- Secondary malignancies
Acute Complications
Life-Threatening Emergencies
Obstructive Complications
Treatment-Related Complications
Surgical Complications Timeline
Early (0-7 days)
- • Bleeding
- • Infection
- • Anastomotic leak
- • Ileus
- • Pneumonia
Intermediate (1-4 weeks)
- • Wound dehiscence
- • Abscess formation
- • Fistula development
- • Delayed gastric emptying
Late (>4 weeks)
- • Adhesions/obstruction
- • Dumping syndrome
- • Nutritional deficiencies
- • Incisional hernia
Chemotherapy-Related Complications
Hematologic Toxicities
- Neutropenia: Infection risk, fever monitoring
- Thrombocytopenia: Bleeding precautions, platelet transfusion
- Anemia: Fatigue, transfusion needs
Non-Hematologic Toxicities
- Cardiotoxicity: Doxorubicin, trastuzumab monitoring
- Nephrotoxicity: Cisplatin, bevacizumab effects
- Neurotoxicity: Oxaliplatin peripheral neuropathy
Long-term Complications
Disease Recurrence
- • Local recurrence: 5-15%
- • Regional recurrence: 10-20%
- • Distant metastases: 20-40%
- • Surveillance imaging
- • Tumor marker monitoring
Secondary Malignancies
- • Radiation-induced cancers
- • Chemotherapy-related leukemia
- • Increased surveillance needs
- • Genetic counseling
- • Lifestyle modifications
Functional Impairment
- • Malabsorption syndromes
- • Chronic pain
- • Sexual dysfunction
- • Psychological distress
- • Quality of life impact
Nursing Surveillance and Prevention
Early Detection Strategies
- • Systematic symptom assessment
- • Vital sign trending
- • Laboratory value monitoring
- • Patient/family education on warning signs
- • Prompt physician communication
Prevention Interventions
- • Evidence-based protocols
- • Prophylactic medications
- • Environmental modifications
- • Patient safety measures
- • Multidisciplinary care coordination
9. Patient Education
Patient Education Framework: “TEACH”
- Tune in to learning needs and readiness
- Edit information to appropriate level
- Act on every teaching moment
- Clarify often and confirm understanding
- Honor the patient as partner in care
Disease Understanding and Prognosis
Essential Knowledge Areas
Disease Process
- • What is cancer?
- • Location and type of tumor
- • Stage and grade explanation
- • Prognosis discussion
- • Treatment goals
Treatment Options
- • Surgery rationale and risks
- • Chemotherapy protocols
- • Radiation therapy plans
- • Targeted therapy options
- • Clinical trial opportunities
Self-Care Management
- • Symptom monitoring
- • Medication compliance
- • Activity limitations
- • When to call healthcare team
- • Emergency situations
Nutrition and Lifestyle Modifications
Nutritional Education Priorities
Dietary Recommendations
- • Lean meats, fish, poultry
- • Eggs, dairy products
- • Legumes, nuts, seeds
- • Protein supplements if needed
- • Healthy fats (avocado, olive oil)
- • Smoothies and shakes
- • Frequent small meals
- • Nutritional supplements
Foods to Avoid/Limit
- • Raw or undercooked foods
- • Unpasteurized products
- • High-fiber foods (if diarrhea)
- • Alcohol and tobacco
- • Processed meats
- • Excessive alcohol
- • High-fat, low-fiber diet
- • Excess refined sugars
Medication Management
Oral Chemotherapy Safety
- • Wear gloves when handling pills
- • Store in original container
- • Keep away from children/pets
- • Do not crush or break tablets
- • Use pill organizers
- • Set medication alarms
- • Keep medication diary
- • Report missed doses
Supportive Medications
- • Take prophylactically
- • Multiple agents may be needed
- • Report breakthrough symptoms
- • Alternative formulations available
- • Around-the-clock dosing
- • Breakthrough pain medications
- • Constipation prevention
- • Non-drug approaches
Psychosocial Support and Resources
Emotional and Social Support
Coping Strategies
- • Stress management techniques
- • Relaxation and meditation
- • Physical activity as tolerated
- • Maintaining social connections
- • Professional counseling
Family Involvement
- • Communication strategies
- • Caregiver support resources
- • Family education sessions
- • Respite care options
- • Children and cancer discussions
Community Resources
- • Cancer support groups
- • Financial assistance programs
- • Transportation services
- • Nutritional programs
- • Complementary therapy options
When to Contact Healthcare Team
Immediate (Emergency)
- • Temperature >100.4°F (38°C)
- • Severe nausea/vomiting preventing fluid intake
- • Signs of dehydration
- • Severe diarrhea (>6 episodes/day)
- • Difficulty breathing
- • Chest pain
- • Severe abdominal pain
Within 24 Hours
- • Persistent nausea despite medications
- • New or worsening pain
- • Unusual fatigue or weakness
- • Changes in bowel/bladder function
- • Skin changes or rash
- • Mood changes or depression
- • Questions about medications
10. Summary & Key Points
Essential Nursing Knowledge: “NURSES CARE”
- Neoplasm understanding and pathophysiology
- Understand treatment modalities
- Recognize complications early
- Systematic symptom assessment
- Educate patients and families
- Coordinate multidisciplinary care
- Advocate for patient needs
- Respect cultural and spiritual beliefs
- Evaluate and improve quality of life
Critical Nursing Competencies
Assessment Skills
- • Comprehensive cancer-focused history
- • Systematic symptom evaluation
- • Nutritional status assessment
- • Psychosocial needs identification
- • Functional status measurement
- • Pain and comfort assessment
Intervention Expertise
- • Chemotherapy administration safety
- • Symptom management protocols
- • Infection prevention measures
- • Patient education delivery
- • Family support facilitation
- • Emergency response readiness
Professional Responsibilities
- • Evidence-based practice application
- • Ethical decision-making support
- • Quality improvement participation
- • Interprofessional collaboration
- • Continuous learning commitment
- • Patient advocacy
GI Tumor Nursing Care Pathway
Comprehensive evaluation, staging, treatment planning
Surgery, chemotherapy, radiation
Symptom management, nutrition
Patient/family teaching
Surveillance, survivorship, palliative care
Evidence-Based Practice Highlights
Enhanced Recovery After Surgery (ERAS)
Multimodal perioperative care pathways designed to achieve early recovery for patients undergoing major surgery.
- • Preoperative counseling and optimization
- • Minimized fasting periods
- • Regional anesthesia techniques
- • Early mobilization and feeding
- • Multimodal pain management
Oral Chemotherapy Management
Systematic approach to ensure safe and effective oral anticancer therapy administration.
- • Standardized patient education protocols
- • Adherence monitoring systems
- • Toxicity assessment tools
- • Healthcare team communication
- • Safe handling procedures
Survivorship Care Planning
Comprehensive approach to long-term care coordination for cancer survivors.
- • Treatment summary documentation
- • Surveillance care plans
- • Late effects monitoring
- • Health promotion strategies
- • Care coordination between providers
Quality Indicators for GI Tumor Nursing Care
Patient Outcomes
- • Reduced hospital readmissions
- • Improved symptom control
- • Enhanced quality of life scores
- • Decreased treatment delays
- • Improved patient satisfaction
Process Measures
- • Timely symptom assessment
- • Appropriate referrals made
- • Education documentation
- • Care plan updates
- • Multidisciplinary collaboration
Continuing Education and Professional Development
Essential Certifications
- • OCN (Oncology Certified Nurse)
- • CBCN (Certified Breast Care Nurse)
- • AOCNP (Advanced Oncology CNP)
- • Chemotherapy/Biotherapy Provider
Professional Organizations
- • Oncology Nursing Society (ONS)
- • Association of Pediatric Hematology/Oncology Nurses
- • International Association for Healthcare Communication
- • American Organization for Nursing Leadership