
Lung Abscess
Comprehensive Nursing Study Guide
Evidence-Based Clinical Knowledge for Nursing Students
Table of Contents
Visual Overview: Lung Abscess Pathophysiology
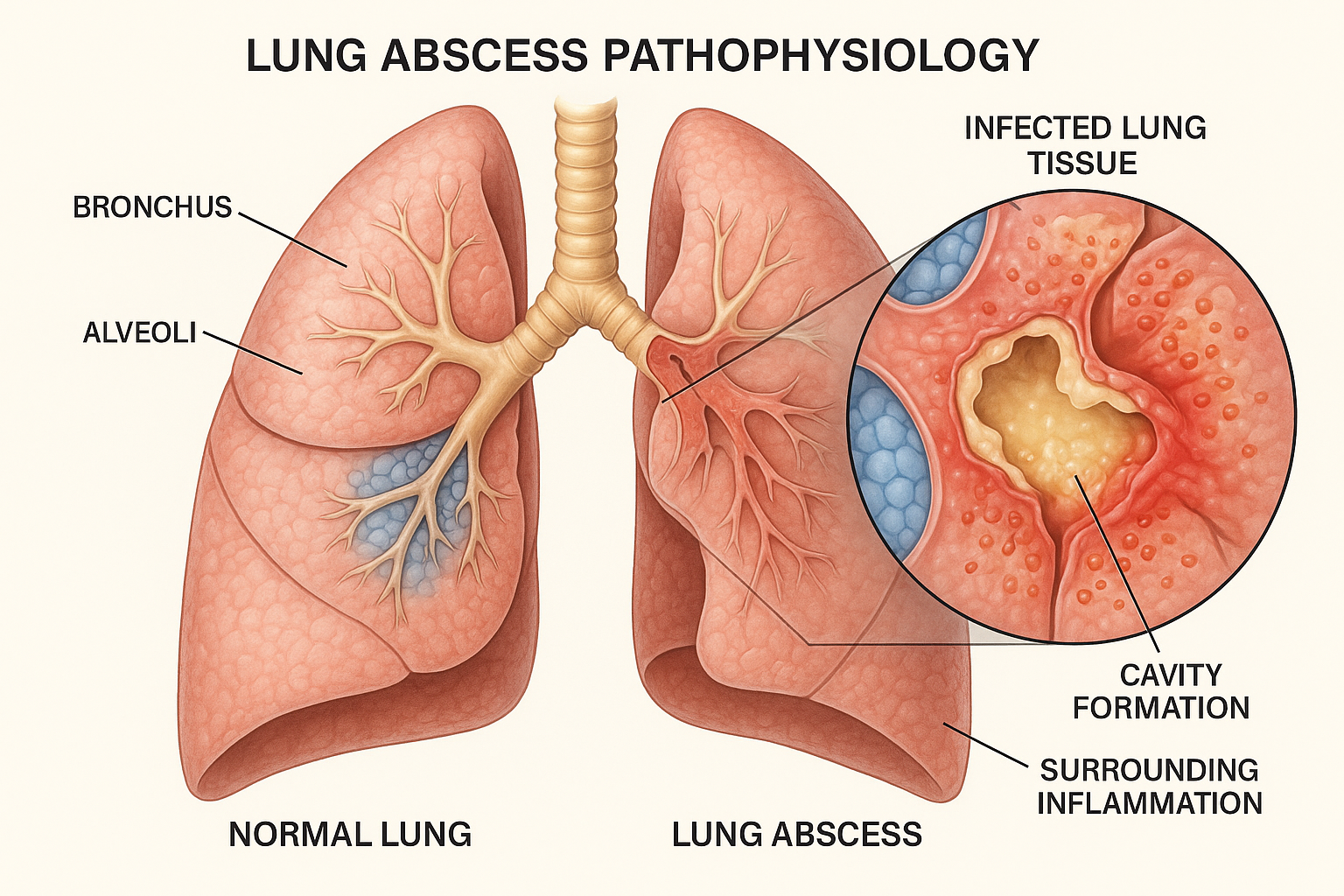
Figure 1: Cross-sectional view showing lung abscess formation with cavity, surrounding inflammation, and comparison to normal lung tissue
1. Definition
A lung abscess is a localized collection of pus within the lung parenchyma, resulting from necrosis of lung tissue caused by microbial infection. This pathological condition represents a severe form of pneumonia characterized by the formation of a thick-walled cavity containing purulent material, typically measuring more than 2 cm in diameter.
Memory Aid – ABSCESS
- Aerobics and Anaerobes (mixed infection)
- Bronchial obstruction
- Sputum production (foul-smelling)
- Cavity formation
- Elevated temperature (fever)
- Severely compromised immunity
- Systemic toxicity
The condition occurs when infectious organisms overwhelm local pulmonary defense mechanisms, leading to tissue necrosis and subsequent cavity formation. Unlike other pneumonic processes, lung abscesses are characterized by their thick, fibrous walls and the presence of air-fluid levels on imaging studies.
2. Types of Lung Abscess
Based on Etiology
Primary Lung Abscess
Occurs in previously healthy individuals with normal lung architecture. Usually caused by aspiration of infected material or community-acquired pathogens.
Secondary Lung Abscess
Develops in patients with underlying lung disease, immunocompromise, or as a complication of pneumonia, bronchial obstruction, or pulmonary embolism.
Based on Duration
Acute Lung Abscess
Duration less than 6 weeks. Characterized by rapid onset of symptoms, high fever, and systemic toxicity. Better prognosis with appropriate treatment.
Chronic Lung Abscess
Duration greater than 6 weeks. Often associated with thick-walled cavities, indolent course, and may require surgical intervention.
3. Etiological Factors
Infectious Agents
Anaerobic Bacteria (70-80%)
- • Bacteroides species
- • Fusobacterium species
- • Peptostreptococcus species
- • Prevotella melaninogenica
Aerobic Bacteria
- • Staphylococcus aureus (including MRSA)
- • Streptococcus pyogenes
- • Klebsiella pneumoniae
- • Pseudomonas aeruginosa
Other Pathogens
- • Mycobacterium tuberculosis
- • Nocardia species
- • Actinomyces israelii
- • Fungal pathogens (immunocompromised)
Risk Factors
Aspiration-Related
- • Alcoholism and substance abuse
- • Neurological disorders (stroke, seizures)
- • Sedation and general anesthesia
- • Poor dental hygiene
- • Dysphagia
Host Factors
- • Immunocompromised states
- • Diabetes mellitus
- • Malignancy
- • Chronic corticosteroid use
- • Malnutrition
Pulmonary Factors
- • Bronchial obstruction
- • COPD
- • Bronchiectasis
- • Pulmonary embolism
- • Lung contusion
4. Pathophysiology
Sequential Pathophysiological Process
Step 1: Initial Infection
Microbial organisms reach lung parenchyma via aspiration, hematogenous spread, or direct extension from adjacent infection.
Step 2: Inflammatory Response
Neutrophil infiltration and release of inflammatory mediators cause localized tissue damage and vascular permeability.
Step 3: Tissue Necrosis
Overwhelming infection leads to ischemia, thrombosis of pulmonary vessels, and subsequent tissue necrosis.
Step 4: Cavity Formation
Necrotic tissue is expectorated through bronchi, leaving behind a cavity filled with pus and necrotic debris.
Step 5: Wall Formation
Surrounding lung tissue develops thick, fibrous walls as a defensive mechanism to contain the infection.
Microbiology
Most lung abscesses are polymicrobial, with anaerobic bacteria predominating. The typical flora consists of oral anaerobes that gain access to the lower respiratory tract through aspiration. The anaerobic environment within the abscess cavity promotes bacterial growth and prevents clearance by host defense mechanisms.
Anatomical Distribution
Aspiration-related abscesses commonly occur in dependent lung segments: posterior segments of upper lobes and superior segments of lower lobes. This distribution reflects the gravitational flow of aspirated material in supine or semi-recumbent positions.
5. Signs and Symptoms
Clinical Presentation Timeline
Early Phase (Days 1-7)
- • High fever (>39°C)
- • Chills and rigors
- • Productive cough
- • Chest pain
- • Malaise
Established Phase (Weeks 1-2)
- • Foul-smelling sputum
- • Hemoptysis
- • Night sweats
- • Weight loss
- • Dyspnea
Chronic Phase (>6 weeks)
- • Persistent cough
- • Cachexia
- • Chronic fatigue
- • Digital clubbing
- • Anemia
Subjective Findings
Cardinal Symptoms
- • Productive cough: Initially purulent, progressing to foul-smelling, putrid sputum
- • Fever: High-grade, often with temperature spikes >39°C
- • Chest pain: Pleuritic in nature, localized to affected area
- • Dyspnea: Progressive, especially on exertion
Associated Symptoms
- • Hemoptysis (20-50% of cases)
- • Night sweats and chills
- • Anorexia and unintentional weight loss
- • Fatigue and malaise
- • Bad breath (halitosis)
Objective Findings
Vital Signs
- • Fever: Often >39°C with rigors
- • Tachycardia: >100 bpm
- • Tachypnea: >20 breaths/min
- • Hypotension (in severe cases)
Physical Examination
- • Inspection: Use of accessory muscles, cyanosis
- • Palpation: Reduced chest expansion over affected area
- • Percussion: Dullness over consolidated areas
- • Auscultation: Decreased breath sounds, rales, rhonchi
- • General: Digital clubbing (chronic cases), lymphadenopathy
6. Assessment
Comprehensive History
Chief Complaint
Document onset, duration, and characteristics of primary symptoms (cough, fever, sputum production)
History of Present Illness
- • Timeline of symptom development
- • Sputum characteristics (color, odor, volume)
- • Fever pattern and associated symptoms
- • Response to previous treatments
Risk Factor Assessment
- • Alcohol or substance abuse history
- • Recent dental procedures or poor oral hygiene
- • History of aspiration or dysphagia
- • Immunocompromising conditions
- • Recent hospitalizations or invasive procedures
Systematic Physical Assessment
General Appearance
- • Level of consciousness and orientation
- • Signs of distress or toxicity
- • Nutritional status
- • Skin color and temperature
Respiratory Assessment
- • Respiratory rate, rhythm, and effort
- • Chest symmetry and expansion
- • Percussion findings
- • Auscultation of all lung fields
- • Assessment for pleural friction rub
Cardiovascular Assessment
- • Heart rate and rhythm
- • Blood pressure and pulse pressure
- • Peripheral perfusion
- • Jugular venous distention
Assessment Tools and Scales
CURB-65 Score
Assess pneumonia severity:
- • Confusion
- • Urea >7 mmol/L
- • Respiratory rate ≥30
- • Blood pressure <90/60
- • Age ≥65 years
SOFA Score
Sequential Organ Failure Assessment for sepsis evaluation
Glasgow Coma Scale
Assess consciousness level if neurological involvement suspected
7. Diagnosis
Laboratory Investigations
Blood Tests
- • Complete Blood Count: Leukocytosis (>12,000/μL), left shift
- • ESR/CRP: Elevated inflammatory markers
- • Blood cultures: Positive in 10-15% of cases
- • Arterial Blood Gas: Hypoxemia, respiratory alkalosis
- • Liver function tests: May be elevated
Sputum Analysis
- • Gram stain: Mixed flora, neutrophil predominance
- • Culture: Often shows mixed anaerobic bacteria
- • Acid-fast bacilli: Rule out tuberculosis
- • Fungal stains: In immunocompromised patients
Imaging Studies
Chest X-ray
- • Thick-walled cavity with air-fluid level
- • Surrounding consolidation
- • Cavity size typically >2 cm diameter
- • May show multiple cavities
CT Chest
- • Better delineation of cavity characteristics
- • Assessment of surrounding lung parenchyma
- • Detection of complications (empyema)
- • Guidance for interventional procedures
Additional Imaging
- • MRI: Rarely used, for specific cases
- • Ultrasound: Assess pleural complications
Diagnostic Criteria
Clinical Criteria
- • Symptoms consistent with lower respiratory tract infection
- • Risk factors for aspiration or immunocompromise
- • Foul-smelling sputum (pathognomonic when present)
- • Failure to respond to standard pneumonia treatment
Radiological Criteria
- • Thick-walled cavity (>4 mm wall thickness)
- • Air-fluid level within cavity
- • Cavity diameter >2 cm
- • Associated consolidation or infiltrates
Differential Diagnosis
Infectious
- • Necrotizing pneumonia
- • Pulmonary tuberculosis
- • Infected pulmonary cyst
- • Septic pulmonary embolism
Neoplastic
- • Primary lung cancer
- • Metastatic disease
- • Cavitating lymphoma
Other
- • Pulmonary infarction
- • Wegener’s granulomatosis
- • Rheumatoid nodules
- • Congenital cystic disease
8. Medical Management
Antimicrobial Therapy
First-Line Treatment
Clindamycin
Dose: 600-900 mg IV q8h or 300-450 mg PO q6h
Duration: 2-4 weeks IV, then oral to complete 6-8 weeks total
Advantages: Excellent anaerobic coverage, good lung penetration
Amoxicillin-Clavulanate
Dose: 875/125 mg PO q12h or 500/125 mg PO q8h
Duration: 6-8 weeks
Advantages: Oral option, broad spectrum
Alternative Regimens
Penicillin G + Metronidazole
Dose: Penicillin G 2-4 million units IV q4-6h + Metronidazole 500 mg IV/PO q8h
Moxifloxacin
Dose: 400 mg IV/PO daily
Note: Reserve for selected cases
Treatment Algorithm
Step 1: Initial Assessment
Evaluate severity, obtain cultures, initiate empirical antibiotics
Step 2: Antibiotic Selection (Day 1-3)
Start clindamycin or amoxicillin-clavulanate based on patient factors
Step 3: Monitoring Response (Day 3-7)
Assess clinical improvement, modify antibiotics if needed
Step 4: Long-term Management (Weeks 2-8)
Continue treatment, consider surgical consultation if no improvement
Supportive Measures
- • Oxygen therapy: Maintain SpO₂ >92%
- • Hydration: Adequate fluid replacement
- • Bronchodilators: For associated bronchospasm
- • Chest physiotherapy: Promote drainage
- • Pain management: Analgesics for pleuritic chest pain
- • Nutritional support: Address malnutrition
Surgical Intervention
Indications
- • Failure of medical therapy after 6-8 weeks
- • Massive hemoptysis
- • Abscess >6 cm diameter
- • Suspected malignancy
- • Empyema development
Procedures
- • Percutaneous drainage
- • Lobectomy or segmentectomy
- • Pneumonectomy (rare)
9. Nursing Management
Priority Nursing Diagnoses
Primary Diagnoses
- 1. Impaired gas exchange related to infectious process
- 2. Ineffective airway clearance related to purulent secretions
- 3. Acute pain related to pleural inflammation
- 4. Risk for infection transmission
Secondary Diagnoses
- 5. Imbalanced nutrition related to anorexia
- 6. Activity intolerance related to hypoxemia
- 7. Anxiety related to respiratory distress
- 8. Deficient knowledge regarding condition
Respiratory Management
Airway Clearance
- • Position patient in semi-Fowler’s or high-Fowler’s position
- • Encourage deep breathing and coughing every 2 hours
- • Perform chest physiotherapy as ordered
- • Use incentive spirometry to prevent atelectasis
- • Suction airway if patient unable to clear secretions
Oxygenation
- • Monitor oxygen saturation continuously
- • Administer supplemental oxygen as prescribed
- • Assess respiratory rate, depth, and effort
- • Monitor arterial blood gases as indicated
Infection Prevention
- • Implement standard precautions consistently
- • Use droplet precautions until TB is ruled out
- • Proper hand hygiene before and after patient contact
- • Dispose of sputum containers appropriately
- • Educate patient on respiratory hygiene/cough etiquette
- • Monitor temperature and vital signs regularly
- • Administer antibiotics as prescribed, monitor for side effects
Holistic Patient Care
Pain Management
- • Assess pain using appropriate pain scales
- • Administer analgesics as prescribed
- • Use non-pharmacological comfort measures
- • Position for comfort and optimal breathing
Nutritional Support
- • Assess nutritional status and intake
- • Provide high-protein, high-calorie diet
- • Encourage small, frequent meals
- • Monitor weight and laboratory values
Patient Education
- • Explain the nature of lung abscess and treatment plan
- • Demonstrate proper coughing techniques
- • Teach importance of medication adherence
- • Discuss signs and symptoms of complications
- • Provide smoking cessation counseling if applicable
- • Explain importance of follow-up care
- • Address concerns about transmission to family members
Key Monitoring Parameters
Vital Signs
- • Temperature q4h
- • Respiratory rate
- • Heart rate
- • Blood pressure
- • Oxygen saturation
Respiratory
- • Breath sounds
- • Work of breathing
- • Sputum characteristics
- • Cough effectiveness
Laboratory
- • White blood cell count
- • C-reactive protein
- • Procalcitonin
- • Blood cultures
General
- • Level of consciousness
- • Nutrition status
- • Fluid balance
- • Activity tolerance
10. Implementation in Nursing Practice
Evidence-Based Nursing Interventions
Research-Supported Interventions
Early Mobilization
Progressive mobility protocols reduce length of stay and improve respiratory outcomes. Start with bed exercises progressing to ambulation as tolerated.
Standardized Assessment Tools
Use validated tools like CURB-65 for severity assessment and NEWS (National Early Warning Score) for deterioration detection.
Structured Communication
Implement SBAR (Situation, Background, Assessment, Recommendation) for effective interprofessional communication.
Quality Improvement Measures
Antibiotic Stewardship
Collaborate with pharmacy to ensure appropriate antibiotic selection, timing, and duration. Monitor for adverse effects and resistance patterns.
Infection Prevention Bundles
Implement ventilator-associated pneumonia prevention bundles and respiratory hygiene protocols to prevent healthcare-associated infections.
Patient Safety Initiatives
Use fall prevention protocols, pressure ulcer prevention, and medication reconciliation processes.
Interdisciplinary Team Collaboration
Medical Team
- • Pulmonologist consultation for complex cases
- • Infectious disease specialist for antibiotic selection
- • Thoracic surgeon for surgical evaluation
- • Intensivist for critically ill patients
Allied Health
- • Respiratory therapist for airway management
- • Clinical pharmacist for medication optimization
- • Dietitian for nutritional assessment
- • Physical therapist for mobility
Support Services
- • Social worker for discharge planning
- • Case manager for care coordination
- • Chaplain for spiritual support
- • Infection control specialist
Clinical Decision-Making Framework
Assessment Phase
Systematic collection of subjective and objective data using evidence-based assessment tools
Analysis Phase
Critical thinking to identify priority problems and nursing diagnoses based on patient data
Planning Phase
Develop individualized care plans with measurable outcomes and evidence-based interventions
Implementation & Evaluation
Execute interventions and continuously evaluate patient response, modifying plan as needed
Core Competencies for Nurses
Clinical Skills
- • Advanced respiratory assessment
- • Airway management techniques
- • Infection control practices
- • Critical thinking and clinical reasoning
Communication Skills
- • Therapeutic communication
- • Patient and family education
- • Interprofessional collaboration
- • Documentation standards
Professional Development
Continuing Education
- • Respiratory care certification programs
- • Infection control training
- • Critical care nursing courses
- • Evidence-based practice workshops
Quality Improvement
- • Participate in quality initiatives
- • Conduct nursing research
- • Mentor new nurses
- • Lead practice improvements
NURSING CARE MNEMONIC: “ABSCESS”
Key Takeaways
Lung abscess represents a serious infectious condition requiring prompt recognition and comprehensive management. As nurses, our role encompasses thorough assessment, evidence-based interventions, patient education, and interdisciplinary collaboration. Early identification of risk factors, particularly aspiration history and immunocompromise, combined with systematic monitoring and individualized care planning, significantly impacts patient outcomes.
Success in managing patients with lung abscess depends on our ability to integrate clinical knowledge with compassionate care, ensuring both immediate safety and long-term recovery. Remember that prolonged antibiotic therapy, typically 6-8 weeks, requires careful monitoring for adherence and side effects, while patient education remains crucial for preventing recurrence and complications.
This comprehensive guide serves as an educational resource for nursing students and practicing nurses. Always consult current clinical guidelines and institutional policies for the most up-to-date practice standards.