
Pleural Effusion
Comprehensive Nursing Notes
Nursing Education
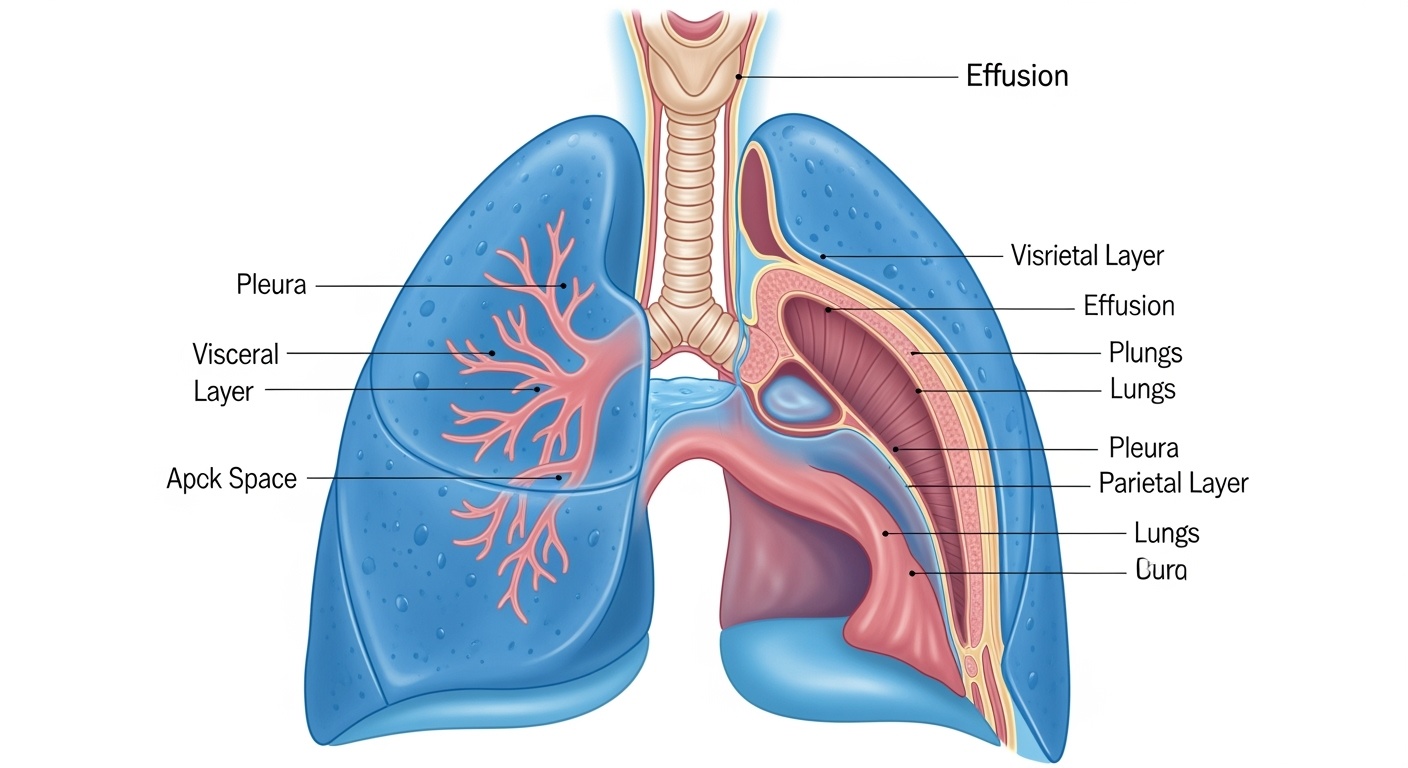
Table of Contents
1. Definition
Pleural effusion is the abnormal accumulation of fluid in the pleural space, the potential cavity between the visceral pleura (covering the lungs) and the parietal pleura (lining the chest wall). Normally, this space contains only 5-15 mL of lubricating fluid that facilitates smooth lung movement during respiration.
Memory Aid: “PLEURA”
- Potential space between lung layers
- Lubricating fluid normally present
- Excess fluid accumulation = effusion
- Under normal conditions: 5-15 mL
- Respiratory compromise when excessive
- Abnormal when >50 mL detectable on X-ray
Clinical Pearl
The pleural space is a “potential” space because the visceral and parietal pleura are normally in close contact. Think of it like two sheets of glass with a thin film of water between them – they slide smoothly but remain together until something separates them.
2. Types & Classification
A. Based on Fluid Characteristics
Transudate
- Low protein content (<3 g/dL)
- Low LDH (<200 IU/L)
- Clear, straw-colored fluid
- Due to systemic factors
- Non-inflammatory
Exudate
- High protein content (>3 g/dL)
- High LDH (>200 IU/L)
- Cloudy, may be colored
- Due to local pleural disease
- Inflammatory process
Light’s Criteria for Exudate
Pleural fluid is exudative if ONE or more criteria are met:
- Pleural fluid protein/serum protein ratio >0.5
- Pleural fluid LDH/serum LDH ratio >0.6
- Pleural fluid LDH >2/3 upper normal serum limit
B. Special Types
Hemothorax
Blood in pleural space (hematocrit >50% of blood hematocrit)
Chylothorax
Lymphatic fluid (triglycerides >110 mg/dL)
Empyema
Infected pleural fluid with pus formation
3. Etiological Factors
A. Transudative Causes
Cardiovascular
- Congestive heart failure (most common)
- Pericardial disease
- Superior vena cava obstruction
Renal/Hepatic
- Nephrotic syndrome
- Cirrhosis with ascites
- Hypoproteinemia
B. Exudative Causes
Infectious
- Pneumonia (parapneumonic)
- Tuberculosis
- Viral infections
- Empyema
- Fungal infections
Malignant
- Lung cancer
- Breast cancer
- Lymphoma
- Mesothelioma
- Metastatic disease
Autoimmune
- Rheumatoid arthritis
- Systemic lupus erythematosus
- Drug-induced lupus
Memory Aid: “HEART CLAMP” for Common Causes
- Heart failure (CHF)
- Empyema/infection
- Autoimmune disorders
- Rheumatoid arthritis
- Tuberculosis
- Cancer/malignancy
- Liver disease (cirrhosis)
- Asbestos (mesothelioma)
- Medications
- Pneumonia (parapneumonic)
4. Pathophysiology
Normal Pleural Fluid Dynamics
Under normal conditions, pleural fluid formation and absorption are in equilibrium:
Pathophysiological Mechanisms
Transudative Mechanism
Exudative Mechanism
Starling’s Law Application
Pleural fluid formation follows Starling’s law of fluid exchange:
Net filtration = K[(Pc – Ppl) – σ(πc – πpl)]
Where disruption of any component can lead to effusion formation.
Compensatory Mechanisms
Respiratory
- Increased respiratory rate
- Use of accessory muscles
- Compensatory hyperventilation
Cardiovascular
- Increased heart rate
- Increased cardiac output
- Venous return alteration
Mechanical
- Mediastinal shift
- Lung compression
- Chest wall adaptation
5. Signs & Symptoms
Critical Alert
Small effusions (<300 mL) may be asymptomatic. Symptoms typically appear when effusion exceeds 500 mL or develops rapidly.
A. Respiratory Symptoms
Primary Symptoms
- Dyspnea: Progressive, exertional initially, then at rest
- Chest pain: Pleuritic, sharp, worse with inspiration
- Cough: Usually dry, nonproductive
- Orthopnea: Difficulty breathing when lying flat
Severity Indicators
- Mild (300-500 mL): Minimal symptoms
- Moderate (500-1500 mL): Dyspnea on exertion
- Severe (>1500 mL): Dyspnea at rest
- Massive (>2000 mL): Respiratory distress
B. Physical Examination Findings
Inspection
- Asymmetrical chest movement
- Affected side expansion ↓
- Tachypnea
- Use of accessory muscles
- Cyanosis (if severe)
Palpation
- Decreased tactile fremitus
- Tracheal deviation (if massive)
- Decreased chest expansion
- Point of maximal impulse shift
Percussion
- Dullness to percussion
- Fluid level may be detected
- Classic “stony dullness”
Auscultation
- Decreased or absent breath sounds
- Bronchial breathing above effusion
- Egophony (E→A changes)
- Pleural friction rub (if inflammatory)
Memory Aid: “DULL” for Physical Findings
- Decreased breath sounds
- Unequal chest expansion
- Less tactile fremitus
- Loud dullness on percussion
C. Associated Symptoms by Etiology
Infectious
- Fever, chills
- Night sweats
- Weight loss
- Productive cough
Malignant
- Weight loss
- Fatigue
- Anorexia
- Chest pain
Heart Failure
- Bilateral pedal edema
- Jugular vein distention
- Paroxysmal nocturnal dyspnea
- S3 gallop
6. Assessment
A. Nursing Assessment Framework
Health History
- Onset: Sudden vs. gradual symptom development
- Duration: Timeline of symptoms
- Severity: Impact on daily activities
- Associated symptoms: Fever, weight loss, night sweats
- Past medical history: CHF, cancer, TB, autoimmune
- Medications: Recent changes, new drugs
- Social history: Smoking, asbestos exposure
Focused Physical Assessment
- Respiratory rate: Note depth, rhythm, effort
- Oxygen saturation: Baseline and with activity
- Blood pressure: Look for pulsus paradoxus
- Heart rate: Tachycardia as compensation
- Temperature: Fever suggests infection
- Weight: Rapid gain suggests fluid retention
- Jugular venous distention: CHF indicator
B. Respiratory Assessment Tools
Systematic Chest Assessment: “IPPA”
C. Functional Assessment
Activity Tolerance
- ADL performance
- Exercise capacity
- Dyspnea scale (0-10)
- Functional status
Quality of Life
- Sleep patterns
- Social interactions
- Emotional well-being
- Work capacity
Risk Factors
- Fall risk (hypoxia)
- Infection risk
- Nutritional status
- Skin integrity
Red Flag Assessments
- Respiratory distress (RR >30)
- Oxygen saturation <88%
- Altered mental status
- Hemodynamic instability
- Worsening dyspnea
- New onset chest pain
- Decreased urine output
- Signs of tension physiology
7. Diagnosis
A. Imaging Studies
Chest X-ray (CXR)
- Upright PA/Lateral: Gold standard initial imaging
- Detection threshold: ~250-500 mL
- Classic findings: Blunted costophrenic angles
- Meniscus sign: Concave fluid meniscus
- Mediastinal shift: Away from effusion (if large)
- Decubitus views: Differentiate free vs. loculated
Ultrasonography
- Detection threshold: ~50 mL
- Real-time guidance: For thoracentesis
- Advantages: Bedside, radiation-free
- Distinguishes: Fluid vs. consolidation
- Loculations: Better than CXR
- BLUE protocol: Rapid assessment tool
Chest X-ray Interpretation Tips
B. Advanced Imaging
CT Chest
- Suspected malignancy
- Complex/loculated effusions
- Empyema evaluation
- Underlying lung pathology
- Detailed anatomy visualization
- Distinguishes pleural masses
- Guides interventions
MRI Chest
- Pleural masses characterization
- Chest wall invasion assessment
- When CT contraindicated
- Motion artifacts
- Cost and availability
- Lengthy procedure
C. Pleural Fluid Analysis
Essential Pleural Fluid Studies: “PLACE”
- Protein and LDH (Light’s criteria)
- Leucocyte count and differential
- Adenopathy workup (cytology if indicated)
- Culture (bacterial, TB, fungal)
- Examination (gross appearance, pH, glucose)
Routine Studies
- Appearance: Clear, cloudy, bloody, milky
- Cell count: WBC <1000 normal
- Protein: Exudate vs. transudate
- LDH: Cellular metabolism marker
- Glucose: Low in infection/malignancy
- pH: <7.30 suggests infection
Specialized Studies
- Cytology: Malignant cells (3 samples)
- Microbiology: Gram stain, cultures
- TB studies: AFB, PCR, culture
- Triglycerides: >110 mg/dL = chylothorax
- Cholesterol: Chronic effusions
- Rheumatoid factor: Autoimmune causes
8. Medical Management
A. Treatment Approach by Etiology
B. Thoracentesis
Indications
- New pleural effusion of unknown etiology
- Suspected infection (empyema)
- Suspected malignancy
- Symptomatic relief (dyspnea)
- Large volume effusion (>1.5 L)
- Respiratory compromise
Contraindications
- Minimal fluid (<10mm on decubitus)
- Bleeding diathesis (uncorrectable)
- Anticoagulation therapy
- Small effusion (<300 mL)
- Mechanical ventilation
- Severe COPD
Safe Thoracentesis Guidelines
- Ultrasound guidance (recommended)
- Coagulation studies if indicated
- Platelet count >50,000
- INR <1.5
- Maximum 1.5 L per session
- Stop if chest pain develops
- Monitor for re-expansion pulmonary edema
- Post-procedure CXR
C. Pharmacological Management
Heart Failure
- Diuretics: Furosemide 40-80mg IV/PO
- ACE inhibitors: Lisinopril 5-20mg daily
- Beta-blockers: Metoprolol 25-100mg BID
- Aldosterone antagonists: Spironolactone 25-50mg
Infection
- Pneumonia: Ceftriaxone + azithromycin
- Empyema: Broad-spectrum antibiotics
- TB: RIPE therapy (6-9 months)
- Antifungals: If fungal etiology
Malignant
- Chemotherapy: Tumor-specific regimens
- Talc pleurodesis: For recurrent effusions
- Corticosteroids: For lymphoma
- Targeted therapy: If appropriate
D. Surgical Interventions
Chest Tube Drainage
- Empyema or complicated parapneumonic effusion
- Recurrent large effusions
- Hemothorax
- Post-thoracentesis pneumothorax
- 28-32 Fr tube typically used
- Water seal drainage system
- Monitor output, air leak
- Daily chest X-rays
Pleurodesis
- Recurrent malignant effusions
- Symptomatic recurrent effusions
- Good functional status patients
- Talc insufflation (VATS)
- Talc slurry (via chest tube)
- Chemical pleurodesis agents
- Success rate: 85-95%
9. Nursing Management
A. Priority Nursing Diagnoses
High Priority
- Impaired gas exchange r/t compression of lung tissue by pleural fluid
- Ineffective breathing pattern r/t decreased lung expansion
- Acute pain r/t pleural inflammation and pressure
- Activity intolerance r/t impaired oxygenation
Secondary Priority
- Anxiety r/t dyspnea and fear of suffocation
- Risk for infection r/t invasive procedures
- Deficient knowledge r/t disease process and treatment
- Risk for falls r/t hypoxia and weakness
B. Nursing Care Planning
SMART Goals Framework
Respiratory Goals
- SaO2 >92% on room air
- RR 12-20 breaths/min
- Clear breath sounds
- Dyspnea scale <4/10
- Normal chest expansion
Comfort Goals
- Pain score <4/10
- Anxiety level manageable
- Able to rest/sleep
- Positioning comfort
- Effective coping
Functional Goals
- Independent ADLs
- Safe ambulation
- Nutritional intake adequate
- Medication compliance
- Knowledge of condition
C. Monitoring and Assessment
Continuous Monitoring Parameters
- Rate, depth, pattern
- Oxygen saturation
- Breath sounds q4h
- Use of accessory muscles
- Heart rate/rhythm
- Blood pressure
- Peripheral pulses
- Capillary refill
- Level of consciousness
- Confusion/restlessness
- Anxiety levels
- Cognitive function
- Temperature
- Skin color/temperature
- Fluid balance
- Pain assessment
Critical Alert Parameters
- RR >30 or <8 breaths/min
- SaO2 <88% despite oxygen
- Systolic BP <90 mmHg
- HR >120 or <50 bpm
- Altered mental status
- Sudden chest pain
- Increased dyspnea
- Subcutaneous emphysema
- Signs of pneumothorax
- Bleeding at procedure site
10. Nursing Implementation
A. Respiratory Support Interventions
Oxygen Therapy
- Assessment: Monitor SaO2, ABGs if ordered
- Delivery methods: Nasal cannula, face mask, high-flow
- Titration: Adjust to maintain SaO2 >92%
- Safety: Fire hazard precautions, skin integrity
- Documentation: FiO2, flow rate, patient response
Positioning Strategies
- Fowler’s position: 45-90° head elevation
- Affected side: Position down to maximize ventilation
- Frequent repositioning: Q2h to prevent complications
- Tripod position: If severe dyspnea
- Comfort measures: Pillows, supports
Breathing Exercises and Techniques
- Place one hand on chest, one on abdomen
- Inhale slowly through nose
- Abdomen should rise more than chest
- Exhale slowly through pursed lips
- Inhale through nose (2 counts)
- Purse lips as if whistling
- Exhale slowly (4 counts)
- Maintains airway pressure
- 10 breaths every hour while awake
- Deep, slow inspirations
- Hold for 3-5 seconds
- Prevents atelectasis
B. Procedure Support and Management
Pre-Thoracentesis Care
- Informed consent: Verify signature, answer questions
- Pre-procedure assessment: Vital signs, allergies
- Laboratory values: PT/PTT, platelets, CBC
- Positioning: Upright, leaning forward on table
- Equipment preparation: Sterile technique setup
- Patient education: Explain procedure, expectations
- Emergency preparedness: Resuscitation equipment nearby
During Thoracentesis
- Patient monitoring: VS q5min, continuous pulse ox
- Positioning assistance: Maintain stable position
- Emotional support: Reassurance, coaching
- Observation: Watch for complications
- Communication: Relay patient concerns to physician
- Specimen handling: Label and send appropriately
- Documentation: Real-time procedure notes
Post-Thoracentesis Complications Monitoring
- Sudden chest pain
- Increased dyspnea
- Asymmetrical chest movement
- Decreased breath sounds
- Cough with frothy sputum
- Chest tightness
- Worsening dyspnea
- Hypoxemia
- Bloody pleural fluid
- Signs of hypovolemia
- Tachycardia, hypotension
- Chest wall hematoma
C. Chest Tube Management
Chest Tube Assessment: “BUBBLE”
- Bubbling in water seal chamber (continuous = air leak)
- Under water seal level (should fluctuate with breathing)
- Blockage assessment (tubing patency)
- Blood/drainage amount and characteristics
- Level of suction if prescribed (-20 cmH2O typical)
- Emergency equipment at bedside
Daily Management
- Drainage measurement: Q8h, note color/consistency
- System integrity: Check connections, tape
- Water levels: Maintain appropriate levels
- Patient positioning: Keep drainage below chest
- Mobility: Encourage early ambulation
- Respiratory therapy: Incentive spirometry
- Pain management: Adequate analgesia
Emergency Interventions
- Cover insertion site with petroleum gauze
- Apply occlusive dressing
- Position patient on affected side
- Call physician immediately
- Monitor vital signs closely
- Assess for hemorrhage
- Notify physician stat
- Prepare for blood transfusion
D. Patient Education and Discharge Planning
Disease Education
- Pathophysiology explanation
- Treatment rationale
- Expected outcomes
- Prognosis discussion
- Risk factor modification
Symptom Management
- When to seek medical care
- Breathing techniques
- Activity modifications
- Pain management strategies
- Energy conservation
Follow-up Care
- Appointment scheduling
- Medication compliance
- Home monitoring
- Support resources
- Emergency contacts
Discharge Readiness Checklist
- Stable vital signs
- Adequate oxygenation on room air
- Pain controlled with oral medications
- No signs of complications
- Chest tube removed (if applicable)
- Demonstrates understanding of condition
- Knows when to seek medical care
- Has support system in place
- Understands medication regimen
- Follow-up appointments scheduled
Call Healthcare Provider If: “SOB-FCP”
- Shortness of breath worsening
- Oxygen saturation dropping
- Blood in sputum or drainage
- Fever >101°F (38.3°C)
- Chest pain increasing
- Pain uncontrolled by medications